



A 52-year-old man with a personal history of vitiligo came to our clinic for assessment of multiple asymptomatic lesions on his upper chest that had first appeared 4 years earlier.
Physical ExaminationPhysical examination revealed 6 soft, oval, hypopigmented, subcutaneous lesions. No follicular component was present but mild friction-induced erythema, without induration, was observed (Fig. 1).
Additional Tests
Dermoscopy showed only achromic macules coinciding with each of the nodules.
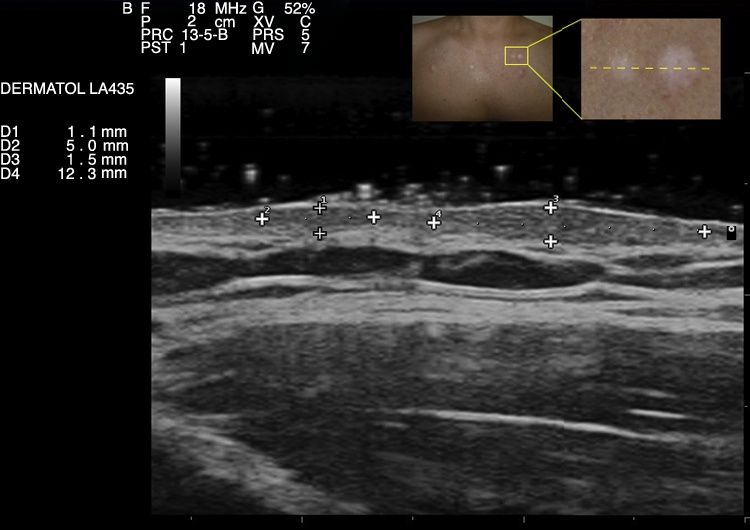
High-frequency ultrasound imaging (18MHz, Esaote MyLabTM25Gold) of 2 contiguous lesions revealed 2 oval foci of thickening and decreased dermal echogenicity that had a solid appearance and were pushing up the epidermis. No sonographic abnormalities of the dermal surface were observed between the 2 foci (Fig. 2). Color Doppler ultrasound showed no sign of vascular flow in the lesions. The other lesions had a similar echostructure.
Histologic examination of a punch biopsy specimen revealed the absence of melanocytes in the basal layer of the epidermis and multiple thin fascicles of smooth muscle fibers oriented in various directions in the middle dermis (Fig. 3).

What Is Your Diagnosis?
DiagnosisMultiple acquired smooth muscle hamartoma (SMH) with vitiligo hypopigmentation.
Clinical Course and TreatmentOne lesion was surgically removed at the patient's request. The other nodules have remained stable over time.
CommentSMH is a rare, benign entity that is slightly more common in men and typically presents as a single congenital lesion; the acquired form is exceptional.1,2
Unlike congenital SMH, the acquired form often does not present hypertrichosis, hyperpigmentation, and pseudo Darier sign. Moreover, while congenital SMH tends to be located on the lumbosacral region and the proximal parts of the limbs, acquired SMH tends to appear on the trunk, neck, upper limbs, vulva, and scrotum.1–3
SMH is mainly diagnosed clinically, although histologic examination may be essential, especially when the clinical presentation is atypical, as in the case of our patient. Histologically, SMH is characterized by the proliferation in the dermis of bundles of smooth muscle oriented in various directions and intermixed with collagen bundles. These bundles, which may or may not be connected to hair follicles, are revealed by histochemical staining with Masson trichrome stain; immunohistochemical techniques such as smooth muscle actin and desmin may also give positive results. Epidermal changes such as acanthosis, papillomatosis, and hypermelanosis can be observed in some cases.3,4 Koizumi et al.5 described CD34-positive dendritic cells in the vicinity of muscle cell bundles in the dermis and interpreted this as a characteristic finding with possible pathogenic implications.
The differential diagnosis is extensive and includes Becker nevus, solitary mastocytoma, connective tissue nevus, and eruptive leiomyoma, among other entities.1,4 Most authors consider Becker nevus and SMH to be polar forms of a spectrum of entities. At one end of the spectrum is Becker nevus, characterized by the predominance of epidermal changes such as hyperpigmentation and hypertrichosis, while at the other end is SMH, characterized by the predominance of smooth muscle cell proliferation over epidermal changes.1–4
Ultrasound findings for this entity are nonspecific, so differential diagnosis must include other soft-tissue tumors with clinical and sonographic similarities, such as dermatofibroma, granuloma annulare, multiple piloleiomyoma, and spontaneous keloids, among other entities. In some cases, we may find differential characteristics that can point to a diagnosis, such as the peripheral hypoechoic lines in dermatofibromas and the hyperechoic linear fibrillar pattern in keloids. However, histopathologic information is often necessary in order to establish a definitive diagnosis.
In conclusion, we have presented an exceptional case of multiple acquired SMH with vitiligo hypopigmentation, probably caused by an isotopic phenomenon. The clinical presentation of SMH in our patient was atypical due to the hypopigmentation, the absence of hypertrichosis, and the multiple lesions, making it necessary to carry out a histopathologic study to confirm the clinical diagnosis. We have also described for the first time the sonographic characteristics of this rare entity. Soft-tissue tumors are a large, heterogeneous group of rare tumors—hence the paucity of information about their sonographic characteristics. We believe that computer-aided diagnostic systems will someday make it easier to distinguish between malignant and benign tumors using high-frequency ultrasound.6
Conflicts of InterestThe authors declare that they have no conflicts of interest.
We would like to thank Dr. Luis Requena Caballero of the dermatology department at Hospital Universitario Fundación Jiménez Díaz.
Please cite this article as: Quintana-Codina M, Melé-Ninot G, Santonja C. Nódulos múltiples hipopigmentados adquiridos en la cara anterior del tórax. Actas Dermosifiliogr. 2018;109:743–744.


