

A 52-year-old woman was referred to our dermatology department in 2015 for the appearance of skin lesions that affected practically her whole left anterior chest wall and neck, proximal area of her left arm, and upper back on the same side. Physical examination revealed an indurated plaque with multiple superficial red-violaceous nodules, and areas of ulceration and necrosis; numerous satellite nodules were also observed on the contralateral chest wall and on the abdomen. In 2005, the patient had been diagnosed with hormone-receptor negative, infiltrating ductal carcinoma of the right breast, with no axillary lymph nodes. This had been treated by conservative surgery with adjuvant hormone therapy (tamoxifen+goserelin) and radiotherapy. Six years later she had presented tumor recurrence with involvement of the contralateral axilla. Total right mastectomy with left axillary lymphadenectomy was therefore performed, followed by radiotherapy and further cycles of chemotherapy between 2011 and 2015 (docetaxel+cyclophosphamide; carboplatin-paclitaxel-bevacizumab; doxorubicina; carboplatin+gemcitabine), but the disease progressed (Fig. 1).
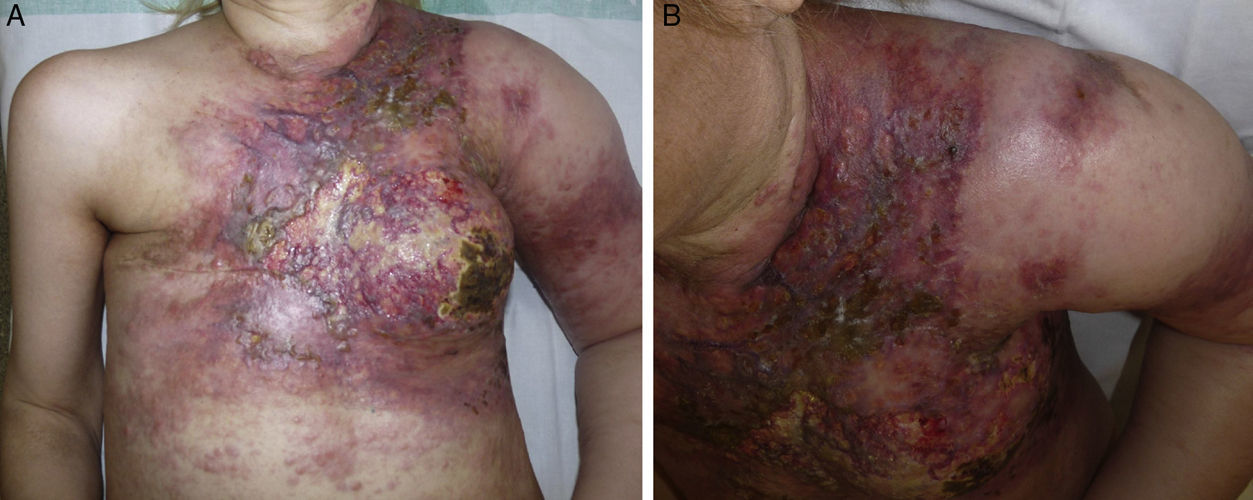
Histopathology revealed lymphangitis carcinomatosa compatible with carcinoma en cuirasse. The patient died 2 months later. Carcinoma en cuirasse was first described by Velpeau in 1838 and is a rare type of skin metastasis with a poor prognosis. It occurs almost exclusively due to tumor infiltration by breast carcinoma.
Please cite this article as: Flores-Terry MA, Romero-Aguilera G, García-Arpa M. Placa indurada con ulceración y necrosis en tórax. Actas Dermosifiliogr. 2017;108:259.


