




A 28-year-old man with no family history of interest presented with asymptomatic nodules on the hands that had first appeared during adolescence. The patient had a history of panhypopituitarism secondary to the excision of a cerebral enchondroma and had undergone surgery to lengthen the right femur and tibia.
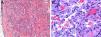
Physical ExaminationPhysical examination revealed 2 types of subcutaneous nodules: some that were soft, mobile, and violaceous, with a vascular appearance (Fig. 1A) and others that were indurated to the touch, nonmobile, and the color of normal skin, suggesting a bone origin (Fig. 1B). Marked scoliosis, dysmetria, and shortening and varus deformity of the right extremities were also present.
Histopathology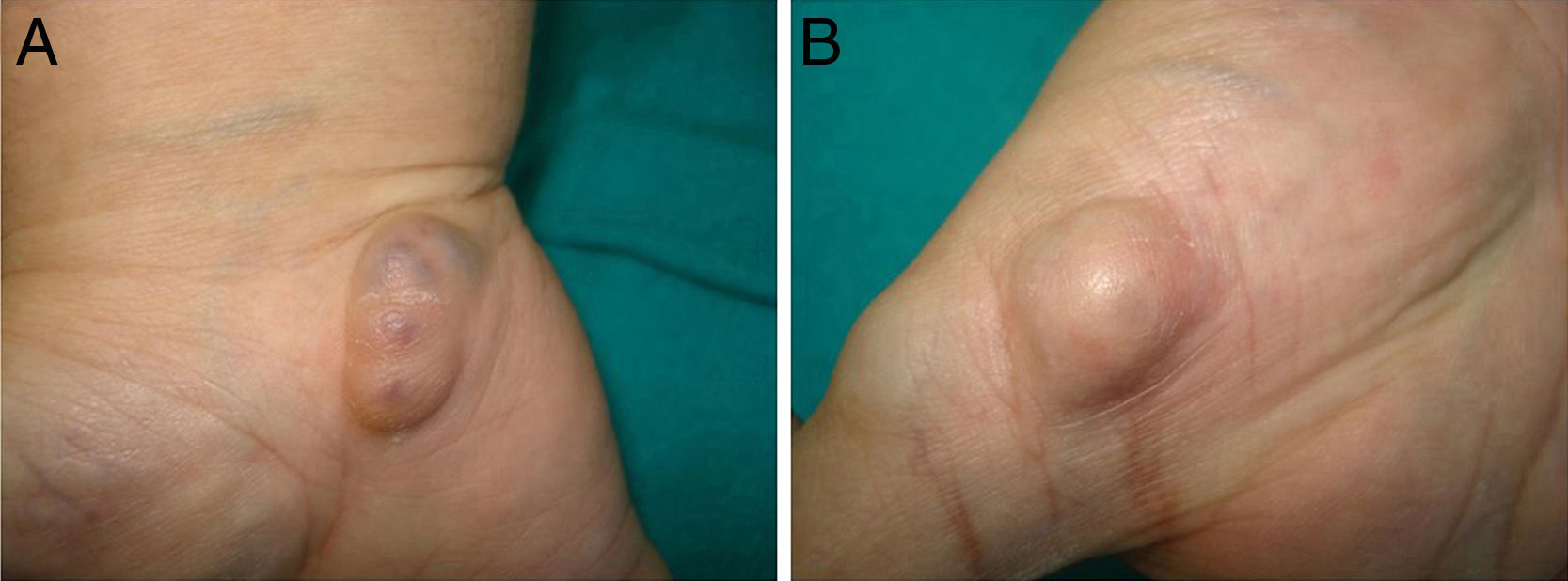
Biopsy of a lesion with a vascular appearance revealed a well-defined nodule in the dermis composed of dilated vascular channels delimited by a thin endothelium. Also present were more solid areas composed of fascicles of spindle cells (Fig. 2A), interspersed with a few round cells with vacuolated cytoplasm (Fig. 2B).
Additional Tests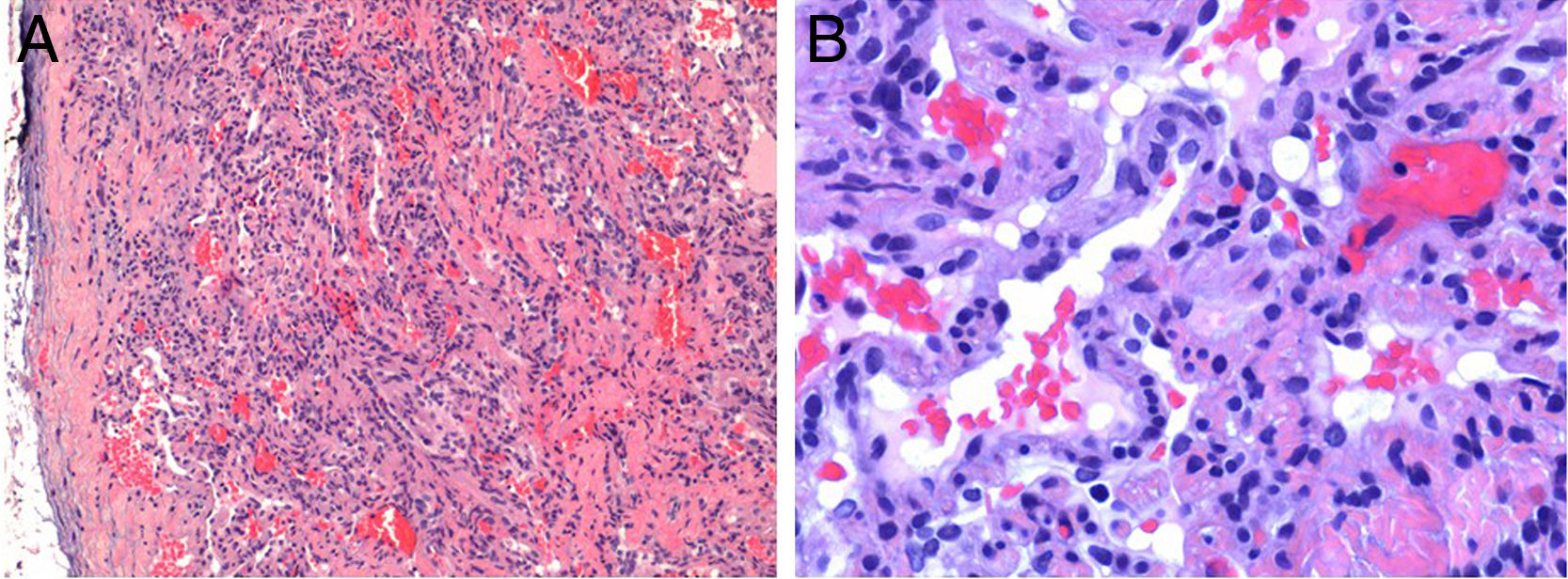
Radiography (Fig. 3A) and magnetic resonance imaging revealed multiple irregular thin-walled images in the phalanges and metacarpals. Bone scintigraphy with technetium-99m hydroxy diphosphonate (99mTc-HDP) revealed multiple foci of increased uptake of the radiotracer, predominantly in the long bones of the right side of the body (Fig. 3B).
What Is Your Diagnosis?
DiagnosisMaffucci syndrome.
Clinical Course and TreatmentAfter 2 years of periodic follow-up visits the patient has not developed any malignancies.
CommentMaffucci syndrome is a rare disorder. Only about 200 cases have been reported since it was first described in 1881. The syndrome is caused by a congenital, nonhereditary mesodermal dysplasia and is characterized by the triad of enchondromas, multiple vascular lesions, and musculoskeletal anomalies.1–6 The etiology is unknown, although recent articles suggest that it could be caused by a postzygotic somatic mutation in the enzymes isocitrate dehydrogenase 1 and 2.2
Patients tend to be asymptomatic at birth and develop lesions in childhood or adolescence. The lesions are distributed asymmetrically, predominantly on one side of the body and on distal parts of the extremities.1–3
Enchondromas are benign cartilaginous tumors clinically characterized as subcutaneous nodules the color of normal skin and with the consistency of bone. Although enchondromas are benign lesions, they can present complications such as deformities or fractures. The most important complication is the possibility of malignant transformation to chondrosarcoma, which occurs in up to 40% of cases. Radiologic studies show irregular images with thin walls that are insufflated but not destroyed and bone scintigraphy shows areas of increased uptake. In most cases, treatment is not necessary except in the event of complications, in which case surgery is the therapeutic option of choice.1–6
The vascular lesions present clinically as soft bluish or violaceous subcutaneous nodules. There are 3 types: venous malformations, lymphatic malformations, and spindle cell hemangioma, the last being the most characteristic type.1–6 Spindle cell hemangioma is a benign vascular proliferation that is histologically composed of 3 components: dilated vascular channels, fascicles of spindle cells, and round cells with vacuolated cytoplasm.3,4 The risk of malignant transformation of the vascular lesions is not established, although it appears to be rare. In fact, only 7 cases of malignant transformation have been reported, specifically 6 angiosarcomas and 1 lymphangiosarcoma, although some of these cases developed at sites exposed to radiotherapy, so the role of radiotherapy in their development is not known.4 Treatment is only required in selected cases and, although surgery is the therapeutic option of choice, recurrences are frequent. In recent years, there have been reports of cases treated with rapamycin, with variable results.5
In addition to the risk of malignant transformation of the enchondromas and vascular lesions, Maffucci syndrome can also be associated with other malignancies such as astrocytomas or pituitary adenomas.6
Therefore, although there are no established follow-up protocols, close monitoring of these patients is essential for early detection of possible neoplasms.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Sanchis-Sánchez C, Mateu-Puchades A, García-Herreros F. Nódulos en las manos y anomalías músculo-esqueléticas. Actas Dermosifiliogr. 2017;108:861–862.


