




A 35-year-old, 135-cm-tall man with healthy consanguineous parents presented with generalized alopecia that had first developed when the patient was 3 months old. The patient had a past history of vitamin D-dependent rickets type II, for which he received treatment with high doses of calcitriol, magnesium, and oral calcium until age 20 years. At age 8 years, the patient developed multiple whitish patches on the scalp. Thereafter, papules gradually appeared on the face, scalp, and forearms and did not respond to topical corticosteroids or oral retinoids.
Physical ExaminationPhysical examination revealed generalized alopecia that spared the eyelashes and a few isolated hairs of the eyebrows. Numerous whitish-yellowish follicular papules were observed on the face, scalp, and forearms (Figs. 1 and 2). No alterations in the nails, teeth, or perspiration were observed.
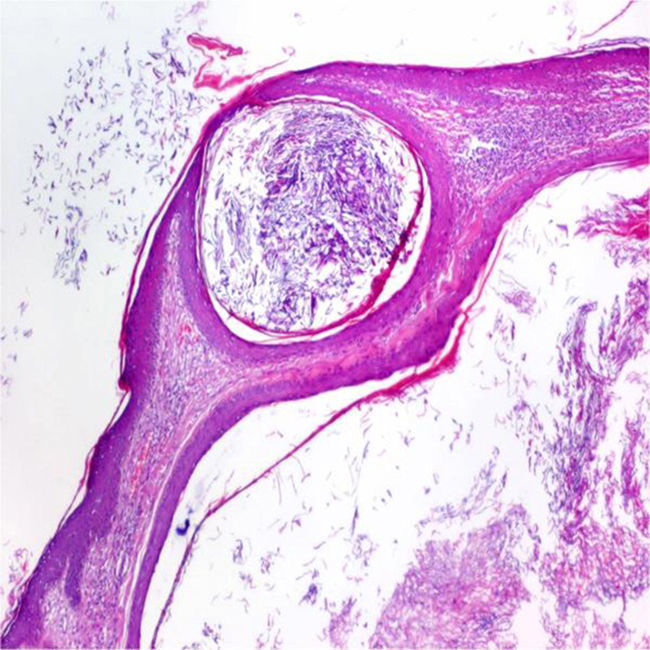
Histopathology

Skin biopsy revealed the presence of keratin-filled cysts in the middle and upper dermis (Fig. 3).
What Is Your Diagnosis?
DiagnosisAlopecia with papular lesions associated with resistant hereditary vitamin D-dependent rickets type II.
Clinical course and treatment: New cysts continued to appear over time. A conservative approach was adopted and symptomatic lesions were surgically removed. A study of the vitamin-D receptor (VDR) gene has not been ordered to date.
CommentResistant vitamin D-dependent rickets type II (VDDR-II) is a rare autosomal recessive genetic disease caused by mutations in the VDR gene.1 Partial or total alopecia is present in 75% of cases.2
Patients with VDDR-II have the same clinical and histologic phenotype as patients with congenital atrichia with papular lesions, which is caused by mutations in the hairless gene.3,4 The hairless and VDR genes participate in the same pathways that regulate the hair cycle. Both diseases entail the separation of the dermal papillae in the first catagen phase of the hair cycle, which leads to the disintegration of the lower two-thirds of the hair follicles and the formation of dermal cysts.5
Hair is present at birth and irreversible alopecia begins in the first months of life. Follicular papules develop on the scalp, face, and extremities in the first few years. In some cases, whitish patches also develop on the scalp. Biopsy reveals an absence of hair follicles and the presence of keratin-filled cysts in the dermis.4,6
It is also important to take into account the family history and history of consanguinity. The main differential diagnosis is alopecia universalis, although genodermatoses associated with hypotrichosis and milia, such as Oley syndrome, Bazex-Dupré-Christol syndrome, and Rombo syndrome, should also be considered.1
Recognition of this entity makes it possible to avoid unnecessary treatments. Moreover, alopecia can precede the onset of symptoms of rickets, so the role of the dermatologist in early diagnosis is of the utmost importance.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: González-Lara L, Gonzalvo-Rodríguez P, Rodríguez-Díaz E. Alopecia, pápulas foliculares y talla baja. Actas Dermosifiliogr. 2017;108:859–860.


