




A 54-year old man with a history of hepatic steatosis presented with stable, asymptomatic lesions on the back of his left hand. They had appeared approximately 10 years earlier, and he had lost the fifth finger of the same hand to an injury 15 years earlier.
Physical ExaminationSeveral papules about 5to6mm in diameter and a reddish–violaceous oval plaque measuring 12×6mm could be seen on physical examination of the back of the hand (Fig. 1). The lesions were slightly infiltrated, well defined, and smooth to the touch.
Histopathology
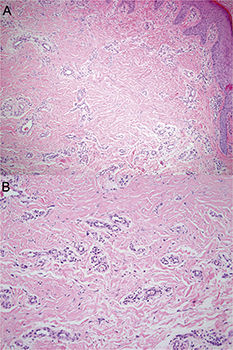
Histopathologic examination showed epidermal acanthosis and many oblong or round small-caliber vessels in the superficial and mid dermis. The vessels were bordered by endothelial cells with prominent nuclei and numerous fibroblasts with angular nuclei among collagen bundles (Fig. 2A). Occasional multinucleated cells (Fig. 2B) were also seen.
Immunohistochemistry revealed intense positive staining of elongated, multinucleated cells for factor XIIIa (Fig. 3), α1-antitrypsin, and lysozyme. Staining with colloidal iron ruled out interstitial mucin deposition.
Additional Tests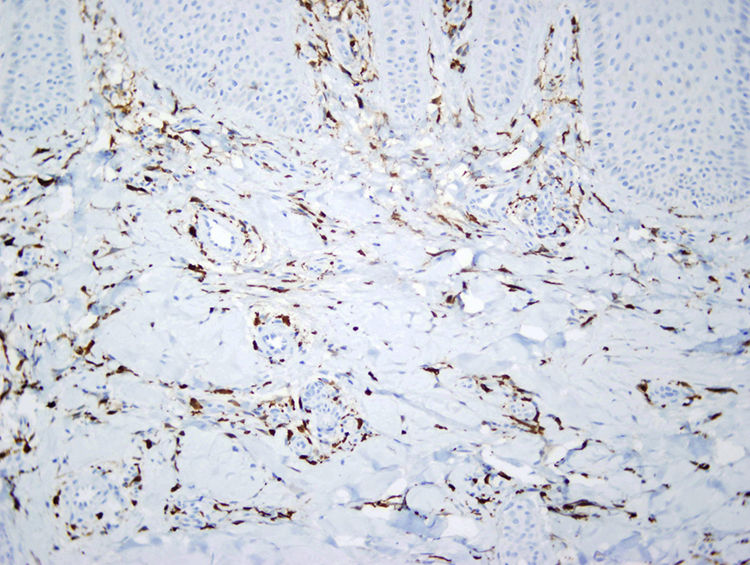
A blood work-up showed elevated glucose levels (151mg/dL) and altered liver function (alanine transaminase, 111U/L; and γ-glutamyltransferase, 182U/L).
What Is Your Diagnosis?
DiagnosisMultinucleate cell angiohistiocytoma.
Clinical Course and TreatmentBecause the lesions were benign and asymptomatic, no treatment was given.
CommentMultinucleate cell angiohistiocytomas are uncommon, benign lesions of uncertain histogenesis. Clinical signs are small, asymptomatic reddish–violaceous papules in acral locations. The lesions are often persistent and typically appear in middle-aged women. Although generalized lesions have been described,1 a bilateral presentation is rare.
These angiohistiocytomas were first described by Smith and Wilson-Jones in 1985,2 and at least 300 cases have since been reported,3 documenting a clinical presentation of small, asymptomatic papules or erythematous–violaceous plaques that grow slowly, are slightly infiltrated, and cluster in a well-defined area. Dermoscopy may reveal whitish patches, finely reticulated areas, and diffuse, poorly defined reddish areas.
The histogenesis of these lesions is uncertain. It is argued that they should be considered fibrohistiocytic tumors, instances of vascular proliferation, or a chronic inflammatory disorder with fibrohistiocytic and vascular hyperplasia.4 Trauma has been suggested as a possible precipitating factor because acral zones are usually involved. A possible role for estrogenic receptors in the development of these lesions has also been hypothesized to explain why they develop mainly in women.5
Histologically, multinucleate cell angiohistiocytomas display a proliferation of capillaries and venules in the upper and mid dermis, prominent endothelial cells accompanied by an infiltrate of lymphocytes and multinucleated cells with angular outlines.The multinucleated interstitial cells express factor XIIIa, vimentin, lysozyme, α1-antitrypsin, and CD68; multinucleated cells usually express only vimentin, although they may also stain for monocyte or macrophage markers.
Differential clinical diagnosis should include granuloma annulare, lichen planus, lymphocytoma, insect bites, sarcoidosis, and Kaposi sarcoma. Differential histologic diagnosis should include dermatofibroma (especially in cases of atrophic vascular histiocytoma) and Kaposi and pseudo-Kaposi sarcomas.
Treatment is usually unnecessary, as the course of disease is benign. However, the literature offers descriptions of good response to cryotherapy as well as argon, carbon dioxide, or 585-nm pulsed-dye laser treatments.6 Surgical excision is also a reasonable step if cosmetic treatment is desired.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Maldonado Seral C, Gómez de Castro C, Vivanco Allende B. Pápulas eritematosas en dorso de mano. Actas Dermosifiliogr. 2019;110:e1–e2.


