




Trichoblastoma is a benign cutaneous neoplasm that is clinically and histologically similar to basal cell carcinoma. We report the dermoscopic features seen in 2 cases of facial trichoblastoma. One case presented with very short, delicate, scarcely branching telangiectases against a pearly white background. In the second case, the veins were also short and scarcely branching, but they were arranged in a crown pattern, with white striae and milia-like cysts. Although dermoscopic evidence of fine, scarcely branching telangiectases is not specific to a diagnosis of trichoblastoma, these features may be useful for differentiating this neoplasm from nodular basal cell carcinoma.
El tricoblastoma es una neoplasia cutánea benigna, con un aspecto clínico e histológico similar al carcinoma basocelular nodular. Comunicamos los hallazgos dermatoscópicos de 2 casos de tricoblastomas localizados en la cara. Un caso presentaba telangiectasias muy finas y cortas, poco ramificadas, sobre un fondo blanquecino perlado. El otro caso mostraba vasos cortos y poco ramificados dispuestos en corona, con estrías blancas y puntos similares a quistes de milium. Aunque las telangiectasias finas y poco ramificadas no son un criterio específico del tricoblastoma, pueden resultar útiles en el diagnóstico diferencial frente al carcinoma basocelular nodular.
Trichoblastoma is a benign cutaneous neoplasm that can appear on any surface with hair follicles, mainly the scalp and face. It generally appears as a solitary nonulcerated flesh-colored nodule measuring 1-2cm and may have superficial telangiectases. Clinically, the differential diagnosis is mainly with basal cell carcinoma.
Case DescriptionsCase 1The patient was a 68-year-old man with a history of multiple basal cell carcinomas on the face. Routine examination revealed a whitish plaque measuring 9mm on the left temple. It had well-defined margins and was poorly infiltrated. Contact polarized light dermoscopy (DermLite FOTO, 3Gen LLC) with ultrasound gel as the interface medium revealed very short and fine telangiectases distributed randomly throughout the lesion on a pearly background (Fig. 1).

Histopathology revealed basal cell nests of various sizes with pilar differentiation in the dermis. There was no contact with the epidermis. The tumor stroma was abundant and contained densely packed fibrocytes (Fig. 2).
Case 2.")
The second patient was a 52-year-old woman who consulted with a 4-mm wheal on her chin that had first appeared 8 months previously. Dermoscopy revealed scarcely branching, radially distributed short vessels arranged in a crown pattern and crossing a ring-like structure with white striae and white spots similar to milia cysts (Fig. 3).

Histopathology revealed basal cell tumor nests throughout the dermis, although there was no contact with the epidermis. The stroma was dense and contained a high number of fibroblasts (Fig. 4).
Discussion.")
Trichoblastoma is a benign cutaneous tumor that differentiates toward hair follicle germinative cells. Trichoepithelioma, desmoplastic trichoepithelioma, and cutaneous lymphadenoma (adamantinoid trichoblastoma) are histopathologic variants of trichoblastoma. Histology reveals follicular papillae and bulbs, as well as abundant stroma containing densely packed fibrocytes.1,2 In clinical and histopathological terms, the differential diagnosis of trichoblastoma is with nodular basal cell carcinoma.
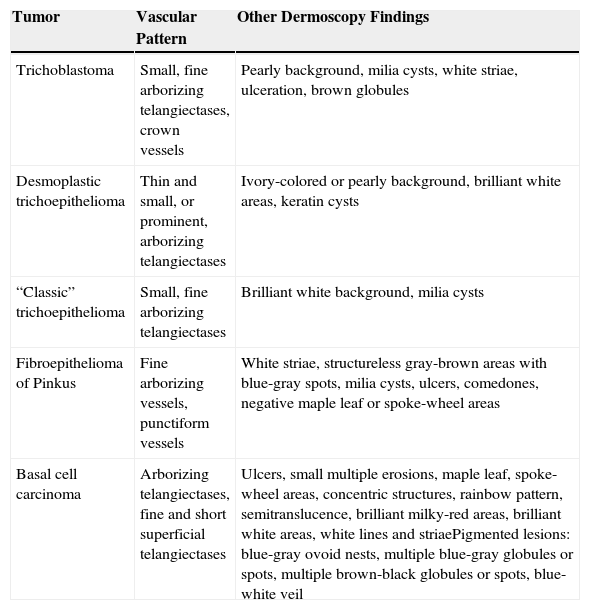
Dermoscopy is very useful for the diagnosis of cutaneous tumors. In the cases reported here, the main dermoscopic structure observed was fine, short, and scarcely branching telangiectases. This structure has been observed in other basal cell skin tumors, such as trichoepithelioma, desmoplastic trichoepithelioma, fibroepithelioma of Pinkus, and, particularly, basal cell carcinoma, as well as in other cutaneous tumors (Table 1).3,4 In a sample of 531 melanocytic and nonmelanocytic cutaneous tumors with a vascular pattern in dermoscopy, branching vessels were described in 82.1% of basal cell carcinomas, 16.7% of sebaceous hyperplasias, 3.2% of dermal or congenital melanocytic nevi, 2.4% of seborrheic keratoses, and 0.7% of melanomas.5 Even though branching telangiectases are a common finding in many cutaneous neoplasms, they are wider in caliber and tend to branch more in nodular basal cell carcinomas, unlike neoplasms included under the term trichoblastoma (trichoblastoma, “classic” trichoepithelioma, and desmoplastic trichoepithelioma), in that they are thin and scarcely branching.6–8 Superficial basal cell carcinoma is also characterized by fine, short telangiectases, generally against a whitish-red background and with multiple small erosions; however, in clinical terms, they are not usually included in the differential diagnosis, since the lesions are flat and nonnodular, like trichoblastomas. The branches in sclerodermiform basal cell carcinoma tend to be finer and less disperse than the arborizing telangiectases that are typical of nodular or cystic basal cell carcinoma. Furthermore, in sclerodermiform basal cell carcinoma, the telangiectases are located on a whitish background with poorly defined margins, in contrast with the translucent, pink, and well-defined background of solid or cystic basal cell carcinoma.9,10 Fibroepithelioma of Pinkus is generally considered a variant of basal cell carcinoma, although some authors feel that it fits better with the concept of “fenestrated” trichoblastoma, or a retiform variant of trichoblastoma, than with basal cell carcinoma.11 Fibroepithelioma of Pinkus is characterized by fine arborizing vessels that are thinner and less branching than the telangiectases of basal cell carcinoma. Whitish striae, the white septal lines corresponding to the intense fibrosis of fibroepithelioma of Pinkus, are very common. Also frequent are the punctiform vessels that are more typical of melanocytic lesions (which in the present case appear on the periphery of the lesion and are always associated with fine arborizing vessels) and milia cysts associated with seborrheic keratosis.12,13 Angiohistiocytoma or intraepidermal poroma may have arborizing telangiectases, even leaf-like structures, that make them almost clinically and dermoscopically identical to basal cell carcinoma.14 Arborizing vessels have also been observed in epidermal cysts, although in these cases, their cystic appearance, the central pore, and the homogeneous color provide clear clues for a correct diagnosis.10
Dermatoscopy Findings for Cutaneous Neoplasms With Branching Telangiectasis.
| Tumor | Vascular Pattern | Other Dermoscopy Findings |
|---|---|---|
| Trichoblastoma | Small, fine arborizing telangiectases, crown vessels | Pearly background, milia cysts, white striae, ulceration, brown globules |
| Desmoplastic trichoepithelioma | Thin and small, or prominent, arborizing telangiectases | Ivory-colored or pearly background, brilliant white areas, keratin cysts |
| “Classic” trichoepithelioma | Small, fine arborizing telangiectases | Brilliant white background, milia cysts |
| Fibroepithelioma of Pinkus | Fine arborizing vessels, punctiform vessels | White striae, structureless gray-brown areas with blue-gray spots, milia cysts, ulcers, comedones, negative maple leaf or spoke-wheel areas |
| Basal cell carcinoma | Arborizing telangiectases, fine and short superficial telangiectases | Ulcers, small multiple erosions, maple leaf, spoke-wheel areas, concentric structures, rainbow pattern, semitranslucence, brilliant milky-red areas, brilliant white areas, white lines and striaePigmented lesions: blue-gray ovoid nests, multiple blue-gray globules or spots, multiple brown-black globules or spots, blue-white veil |
The trichoblastomas described here also had crown vessels, a pearly background, milia cysts, and brilliant white striae. Given that these dermoscopy findings have also been reported in other basal cell skin tumors, no single dermoscopic finding can be considered pathognomic of trichoblastoma.
The white structures observed in the cases of trichoblastoma we report seem to reflect the dermatoscopic image of their densely fibrous stroma, as is the case in trichoepithelioma, fibroepithelioma of Pinkus, and sclerodermiform basal cell carcinoma. Compared with the brilliant white background of the “classic” trichoepitheliomas, the pearly or ivory-colored background could be characteristic of desmoplastic trichoepithelioma; however, this finding is difficult to differentiate using dermoscopy, and interobserver agreement has never been assessed.15
ConclusionsThe dermoscopy findings in the 2 cases of trichoblastoma described here have been observed in other basal cell neoplasms, such as trichoepithelioma, desmoplastic trichoepithelioma, fibroepithelioma of Pinkus, and, more commonly, basal cell carcinoma. The only dermoscopy finding common to the 2 cases was the presence of fine, short, poorly branching telangiectases. Although this vascular pattern has been observed in various neoplasms that are clinically similar to trichoblastoma, it could prove useful for differentiating this neoplasm from nodular basal cell carcinoma.
Ethical DisclosuresProtection of Persons and AnimalsThe authors declare that this research did not involve experiments performed on humans or animals.
Confidentiality of DataThe authors declare that they have followed their hospital's protocol on the publication of data concerning patients.
Right to privacy and informed consentThe authors declare that no private patient data are disclosed in this article.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Pitarch G, Botella-Estrada R. Dermatoscopia del tricoblastoma. Actas Dermosifiliogr. 2015;106:e45–e48.



