






An 84-year-old woman with a history of osteoporosis, systemic hypertension, dyslipidemia, and surgical excision of a basal cell carcinoma on the face was seen in our dermatology outpatients for evaluation of a lesion on the anteromedial aspect of the right knee. The lesion had appeared a year earlier, 2 months after prosthetic knee replacement, and had progressively increased in size. It was asymptomatic.
Physical ExaminationOn physical examination, a tuberous erythematous lesion measuring 3.5×1cm and of friable appearance was observed on the anteromedial aspect of the right knee (Fig. 1). There were no palpable locoregional lymph nodes.
Histopathology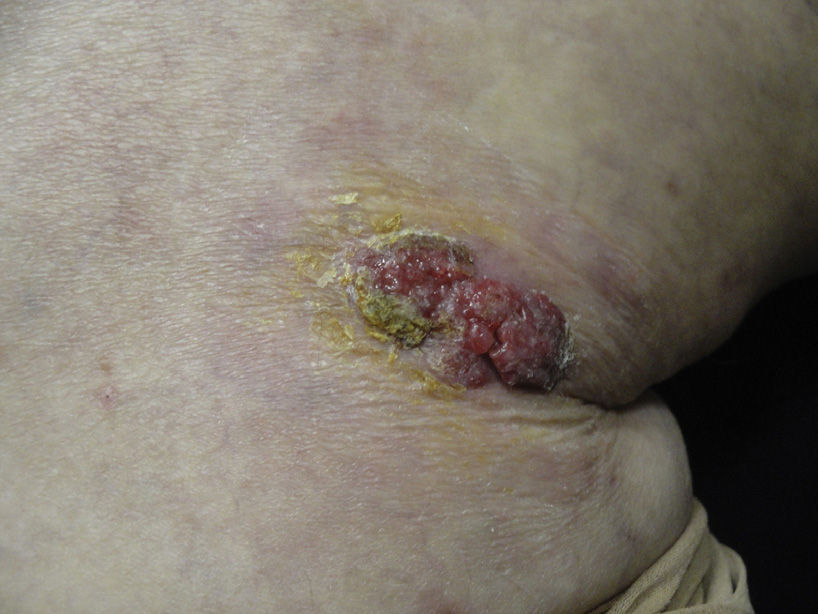
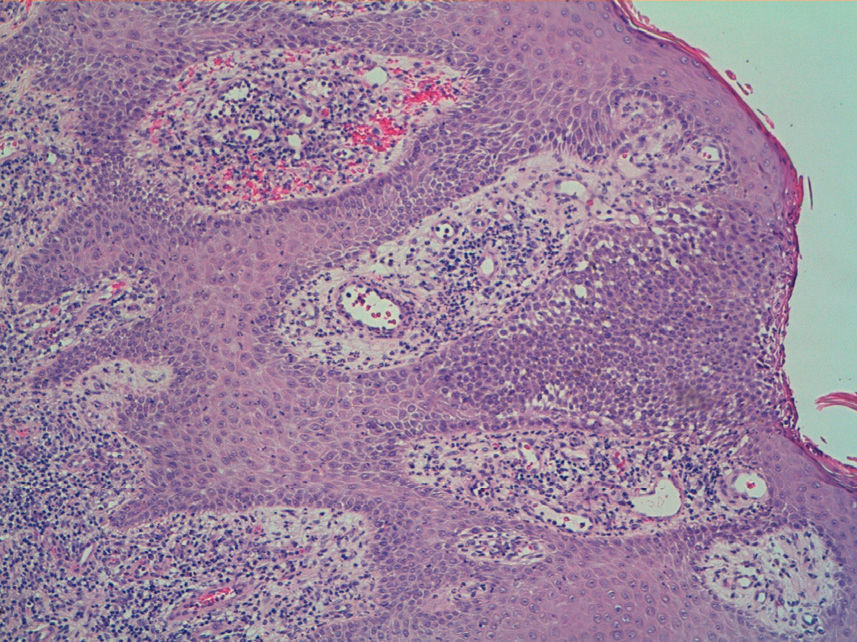
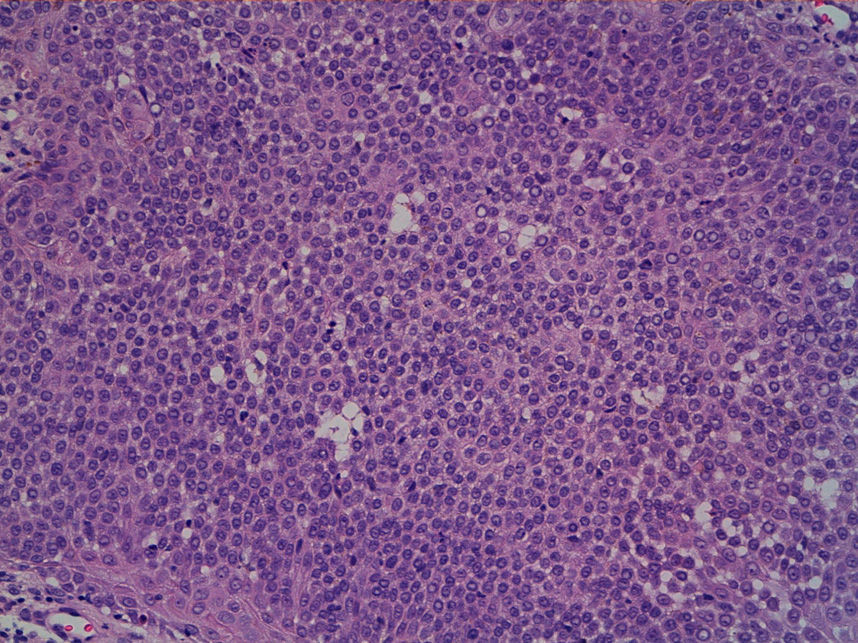
Biopsy of the lesion revealed an acanthotic and hyperkeratotic epidermis in which circumscribed nests of cells with a basaloid appearance were observed (Fig. 2). These nests were formed of a proliferation of monomorphic cuboidal or oval cells and contained ductal structures (Fig. 3). Immunohistochemistry was positive for epithelial membrane antigen and negative for carcinoembryonic antigen and S-100.
What Is Your Diagnosis?
DiagnosisHidroacanthoma simplex (HS).
Clinical Course and TreatmentComplete surgical excision of the lesion was performed and the clinical course was favorable, with no signs of recurrence at 6 months.
CommentPoromas are benign tumors with ductal differentiation. They are formed of 2 different cell types: poroid cells, with round basophilic nuclei and scant cytoplasm, similar to the cells of the peripheral layer of the distal segment of eccrine or apocrine ducts; and cuticular cells, which are larger and have abundant eosinophilic cytoplasm, similar to the luminal cells of the ductal segment of the ducts. Four tumor types are distinguished according to the architecture of the neoplasm: HS, classic poroma, poroid hidradenoma, and dermal duct tumor (Table 1). The etiology of these tumors is unknown.
Classification of the Poromas According to Their Architectural Pattern.
| Type of Eccrine Poroma | Distribution of the Neoplastic Cells in the Dermis and Epidermis |
|---|---|
| Hidroacanthoma simplex | Intraepidermal nests of neoplastic cells of round or oval morphology |
| Classic poroma | Cords and islets of neoplastic cells that make contact with the epidermis and infiltrate the superficial dermis |
| Dermal duct tumor | Small nodules of neoplastic cells scattered through the dermis, showing no connection with the epidermis and no evidence of cyst formation |
| Poroid hidradenoma | Solitary or limited number of nodules of neoplastic cells in the dermis, larger than eccrine duct nodules, with solid and cystic components |
HS was described by Smith and Coburn1 in 1956 as a benign intraepidermal tumor arising from the sweat glands. It is a rare tumor with no distinctive clinical characteristics and it can be confused with a wide variety of other lesions, such as seborrheic keratosis, basal cell carcinoma, and Bowen disease. It is most common on the limbs, particularly the legs, although it has also been reported at other sites, including the trunk, arms, and head and neck.2 This tumor typically occurs in elderly individuals and affects both sexes equally.
The 4 types of poroma have common histologic features and are derived from the basal keratinocytes of the most distal segment of the eccrine duct.3 HS is formed of intraepidermal nests of round or oval neoplastic cells in an irregularly acanthotic epidermis. It is 1 of the tumors in which the Borst-Jadassohn phenomenon (epidermal aggregates of basaloid cells) can be observed; this phenomenon can also be seen in clonal seborrheic keratosis, Bowen disease, melanomas, and eccrine porocarcinoma. On immunohistochemical analysis, HS tumor cells usually express epithelial membrane antigen but not carcinoembryonic antigen or S-100.
Dermoscopy can help in the clinical diagnosis of poromas. The vascular pattern is the most useful dermoscopic feature.4 A polymorphous vascular pattern is most commonly observed, with irregular milky-red areas, red lacunae, irregular linear vessels, and branching vessels with elliptical and semielliptical endings that have been called “leaf and flower-like” vessels, a pattern unique to poromas. Furthermore, the vessels in a poroma are usually less clear than the branching vessels of basal cell carcinoma, which would suggest that these vessels are situated deeper in the dermis in poroma.5
Eccrine porocarcinoma, also called in situ porocarcinoma or malignant HS, is the malignant variant of HS.6 This tumor typically shows greater nuclear and cytoplasmic pleomorphism, prominent nucleoli, and a large number of mitoses.
As HS is a benign tumor, its prognosis is favorable, and complete surgical excision is the curative treatment of choice.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Eguren C, Burdaspal A, de la Cueva-Dobao P. Lesión tuberosa en la rodilla de un año de evolución. Actas Dermosifiliogr. 2016;107:517–518.


