


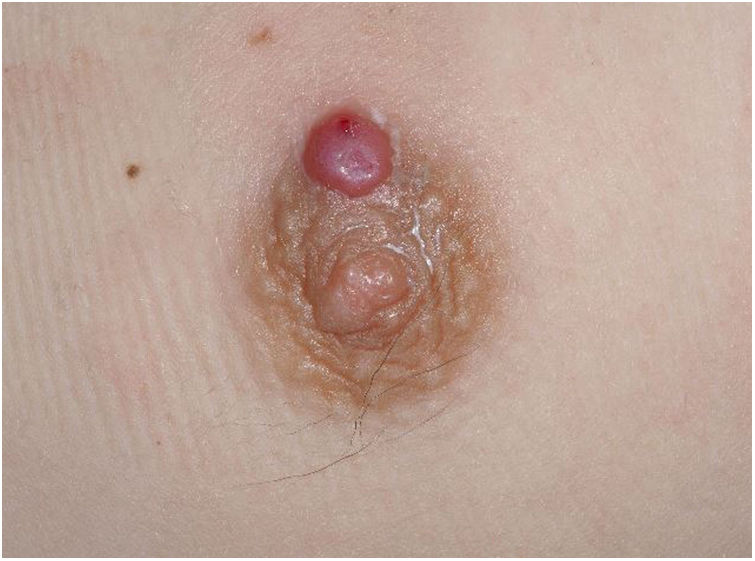
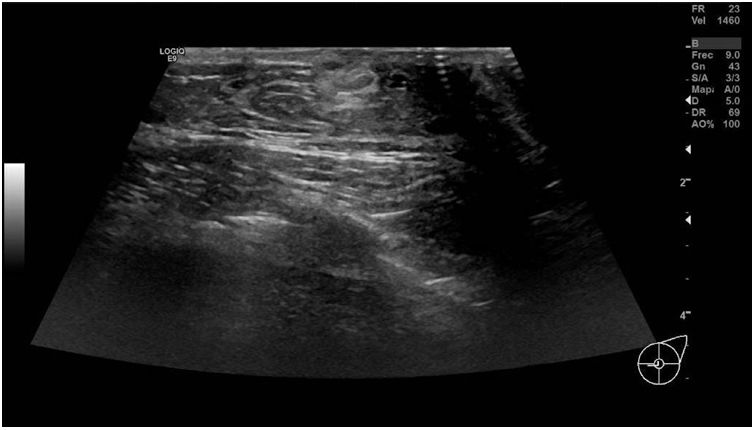
A healthy 13-year-old male presented with an inflammatory lesion on the left areola that had appeared approximately 3 weeks earlier. An indurated plaque was palpable in the area of the left breast, and drained purulent material under pressure (Fig. 1). Bacteriological study of the drained material revealed the presence of Staphylococcus aureus sensitive to amoxicillin–clavulanic acid. To confirm the diagnosis, the patient underwent bilateral breast ultrasound, which showed gynecomastia in both breasts accompanied by small cystic lesions on the left side (Fig. 2). A Montgomery gland, with inflammatory changes and no drainable material, was identified in the left areola, medial to the nipple.
What is your Diagnosis?
DiagnosisMontgomery or retroareolar cyst.
Clinical Course and TreatmentThe clinical picture resolved after treatment with betamethasone (0.5 mg/g) and topical gentamicin (1 mg/g) for 10 days.
CommentMontgomery cyst is a rare entity in female adolescents and is even less frequent in males. Its true incidence is unknown, and the published literature is scant.
The cyst forms due to obstruction and dilation of the Montgomery tubercle, a sebaceous gland closely connected to the terminal portion of the lactiferous duct.1 Several hypotheses have been proposed to explain the mechanism by which these ducts are obstructed and dilated. These include ineffective absorption of secretions, squamous metaplasia of the duct surface, primary autoimmune dilation of the duct, and hormonally induced relaxation of the areolar muscle.2
The clinical presentation can be symptomatic or asymptomatic. The symptomatic form is more common, presenting as an inflammatory retroareolar mass with pain and erythema. It can be unilateral or bilateral (up to 50% of cases), and is occasionally associated with a serous, milky, or brownish discharge from the nipple.3,4
Breast ultrasound is the technique of choice both for diagnosis and follow-up. In some cases, typically those involving inflammation, the cyst may present levels or septa and increased peripheral vascularity, which is observed using the Doppler technique.4,5
It is important to include retroareolar abscess in the differential diagnosis of Montgomery cyst. Abscesses tend to be more fluctuating or indurated, and are more likely to be accompanied by systemic symptoms. Resolution of abscesses requires draining, whereas Montgomery cysts have a benign course, and respond well to antibiotic and anti-inflammatory treatment.2,4 Nonetheless, it should be noted that retroareolar cysts can evolve to abscesses, although this is rare.2 Another condition included in the differential diagnosis is lymphangioma, owing to the bluish appearance of the retroareolar mass.
Treatment usually consists of outpatient oral antibiotic therapy with amoxicillin–clavulanic acid, and nonsteroidal anti-inflammatories in cases of inflamed cysts.5 Because the cysts respond well to the appropriate treatment, incision and drainage are not recommended. Drainage should be reserved for cysts that do not respond to treatment and evolve to abscesses, or those in which ultrasound findings suggest malignancy.1,4 Symptomatic retroareolar cysts should be followed up 7 days after starting treatment to confirm resolution or a reduction in size. Asymptomatic cysts usually resolve spontaneously, although ultrasound follow-up is also recommended.4
Conflicts of InterestThe authors declare that they have no conflicts of interest.


