
Mycosis fungoides and cutaneous anaplastic large-cell lymphoma (CALCL) are primary T-cell lymphomas. Prognosis is good in the initial stages, and the wide range of available first-line treatments includes topical corticosteroids, phototherapy, localized radiotherapy, and mechlorethamine. Survival is lower and quality of life considerably affected in advanced stages. The recommended treatment options include bexarotene, methotrexate, interferon, chemotherapy, and radiotherapy.1
Brentuximab is a monoclonal antibody that targets CD30 (Table 1). It is approved by the United States Food and Drug Administration (FDA) for the treatment of Hodgkin lymphoma that is refractory to chemotherapy and autologous hematopoietic stem cell transplant and for the treatment of refractory anaplastic large-cell lymphoma.2 The FDA recently approved its use in mycosis fungoides with expression of CD30 (MF-CD30+) and in CALCL-CD30+ based on the results of a phase 3 multicenter randomized clinical trial, ALCANZA,3 which included 131 patients with MF-CD30+ (n = 97), CD30 expression >10%, or CALCL (n = 31) who had previously been treated with systemic agents or radiotherapy. The intention-to-treat analysis included 128 individuals (3 were excluded because of CD30 expression <10%). Of these, 64 received brentuximab (16 cycles of 1.8mg/kg every 3 wk) and 64 received therapy chosen by the attending physician (physician's choice) with oral bexarotene (300mg/m2/d) or methotrexate (5-50mg/wk) for up to 48 weeks. The primary endpoint was the percentage of patients achieving an objective global response lasting at least 4 months. After a mean follow-up of almost 2 years (22.9mo), the objective overall response at 4 months was 56.3% in the brentuximab group compared with 12.5% in the physician's choice group (P<.0001). Complete response was 16% in the brentuximab group compared with 2% in the physician's choice group (P<.0046). Progression-free survival was also higher with brentuximab (16.7 vs 3.5mo in the physician's choice group), as was symptom relief. The outcome of treatment with brentuximab was better than that of bexarotene or methotrexate, irrespective of age, sex, type of cutaneous T-cell lymphoma (MF-CD30+ or CALCL), and involvement (cutaneous vs visceral-cutaneous).
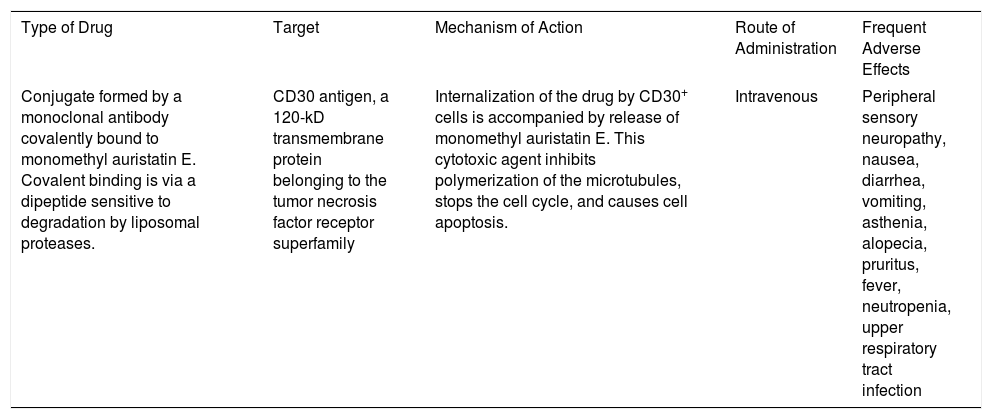
Characteristics of Brentuximab.
| Type of Drug | Target | Mechanism of Action | Route of Administration | Frequent Adverse Effects |
|---|---|---|---|---|
| Conjugate formed by a monoclonal antibody covalently bound to monomethyl auristatin E. Covalent binding is via a dipeptide sensitive to degradation by liposomal proteases. | CD30 antigen, a 120-kD transmembrane protein belonging to the tumor necrosis factor receptor superfamily | Internalization of the drug by CD30+ cells is accompanied by release of monomethyl auristatin E. This cytotoxic agent inhibits polymerization of the microtubules, stops the cell cycle, and causes cell apoptosis. | Intravenous | Peripheral sensory neuropathy, nausea, diarrhea, vomiting, asthenia, alopecia, pruritus, fever, neutropenia, upper respiratory tract infection |
The frequency of adverse events was 29% in both groups. In the brentuximab group, 24% of patients had to suspend treatment because of adverse events compared with 8% in the physician's choice group. Peripheral neuropathy was the most frequent toxicity (67%) with brentuximab. Symptoms improved during posttreatment follow-up in 82% of those affected.
CD30 expression is variable in mycosis fungoides, and there is no consensus on the minimum threshold necessary to obtain a clinical response with brentuximab. A phase 2 study with this agent revealed clinical responses even with CD30 expression <5% (response rate of 17%), although greater response rates (up to 83%) were observed in those cases of mycosis fungoides with expression >5%.4 In another phase 2 study, Duvic et al.5 found no differences in response between patients with low expression (<10%) and high expression of CD30. In a recent report, a patient with CD30-negative mycosis fungoides (CD30 <1%) that was refractory to multiple treatment lines achieved a complete response with brentuximab.6
As for dosing, a recent systematic review showed that lower doses of brentuximab (1.2mg/kg every 3 wk) could be equally effective, with fewer adverse effects.7
Brentuximab has proven to be superior to habitual treatments for advanced phase CD30-positive cutaneous large-cell lymphoma, although questions remain concerning the minimum threshold of CD30 expression for the therapy to be considered effective. Dermatologists should make every effort to become familiar with the growing list of currently available biologics. We believe that this new alternative therapy will prolong the survival of patients with advanced CD30-positive cutaneous T-cell lymphoma, although its high cost is a major limitation to its use.
Please cite this article as: Morgado-Carrasco D, Combalia A, Estrach Panella T. FR - Brentuximab como tratamiento de los linfomas cutáneos primarios CD30 Eczema y urticaria en Portugal. 2019;110:769–770.



