







The cheek is the largest anatomical subunit of the face. It is a bilateral structure and symmetry must therefore be preserved. Peripherally it is related to important natural orifices whose location must also be maintained during surgical reconstructions. This is particularly important in the medial zygomatic subunit, whose delicate junction with the lower eyelid means that care must be taken to avoid ectropion. We present 5 options for the reconstruction of surgical defects secondary to the excision of tumors in this region.
La mejilla es la subunidad anatómica mayor de la cara. Es una estructura bilateral, por lo que es necesario respetar la simetría. Por otra parte contacta periféricamente con importantes orificios naturales cuya localización debemos respetar en la reconstrucción quirúrgica. Esto es particularmente importante en la subunidad cigomático-medial, cuya delicada unión con el párpado inferior hace que tengamos que ser cuidadosos para evitar un ectropión. Presentamos 5 opciones reconstructivas de defectos quirúrgicos secundarios a la extirpación de otros tantos tumores en esta localización.
The cheek is the largest cosmetic unit of the face. It has clear limits defined by the zygomatic arch and the infraorbital rim superiorly, the nasolabial and melolabial folds medially, the mandibular border inferiorly, and the preauricular region laterally. For educational purposes, it is classically divided into 4 cosmetic subunits: medial, zygomatic, buccal, and lateral.1 Each of these subunits has specific characteristics that the surgeon must take into account during reconstruction procedures in order to achieve the best functional and cosmetic outcome. Ideally, incisions and borders of flaps should be situated within these subunits to best camouflage the resulting scars. We evaluate a number of reconstruction techniques in patients with tumors situated in the medial and zygomatic regions.2
In the medial subunit we must take into account that the union of the cheek with the eyelid forms its own subunit, and we must also therefore respect the position and function of the lower eyelid, as well as the morphology of this subunit and the gradual change that occurs from the malar to the palpebral regions.3
The zygomatic ligament fixes the skin of the zygomatic subunit, and it must be remembered during surgery that the temporal branch of the facial nerve is in a very superficial plane in this region.
Reconstruction of the malar eminence must respect the fat pad, which creates the convexity of this area and gives it volume.2
The blood supply is derived from the facial artery and its branches, motor innervation is via the facial nerve, and the sensory supply is from the maxillary nerve, a branch of the fifth cranial nerve.3
Case DescriptionsCase 1The patient was a 75-year-old woman with a lentigo maligna melanoma of 2.2×1.2cm. After resection of the lesion, an advancement-rotation flap was designed above the zygomatic arch, extending to tragus. The inferior border of the defect was triangulated and a Z-plasty was used in the preauricular region to allow greater advancement of the flap. The subcutaneous tissue was sutured with Vicryl and the skin was closed with 4/0 silk (Fig. 1).
Case 2
A man aged 78 years presented a basal cell carcinoma of 1.6×0.8cm on the lateral third of the upper left eyelid and a lentigo maligna melanoma of 3×4cm on the left cheek. After excision of the cheek lesion, an advancement flap was designed in the temporal region. The superomedial border of the defect was triangulated, the inferior border was undermined, and the eyelid tumor was excised using a triangular incision, which served as a tension-releasing triangle for advancement of the flap. The skin was sutured with 4/0 silk (Fig. 2).
Case 3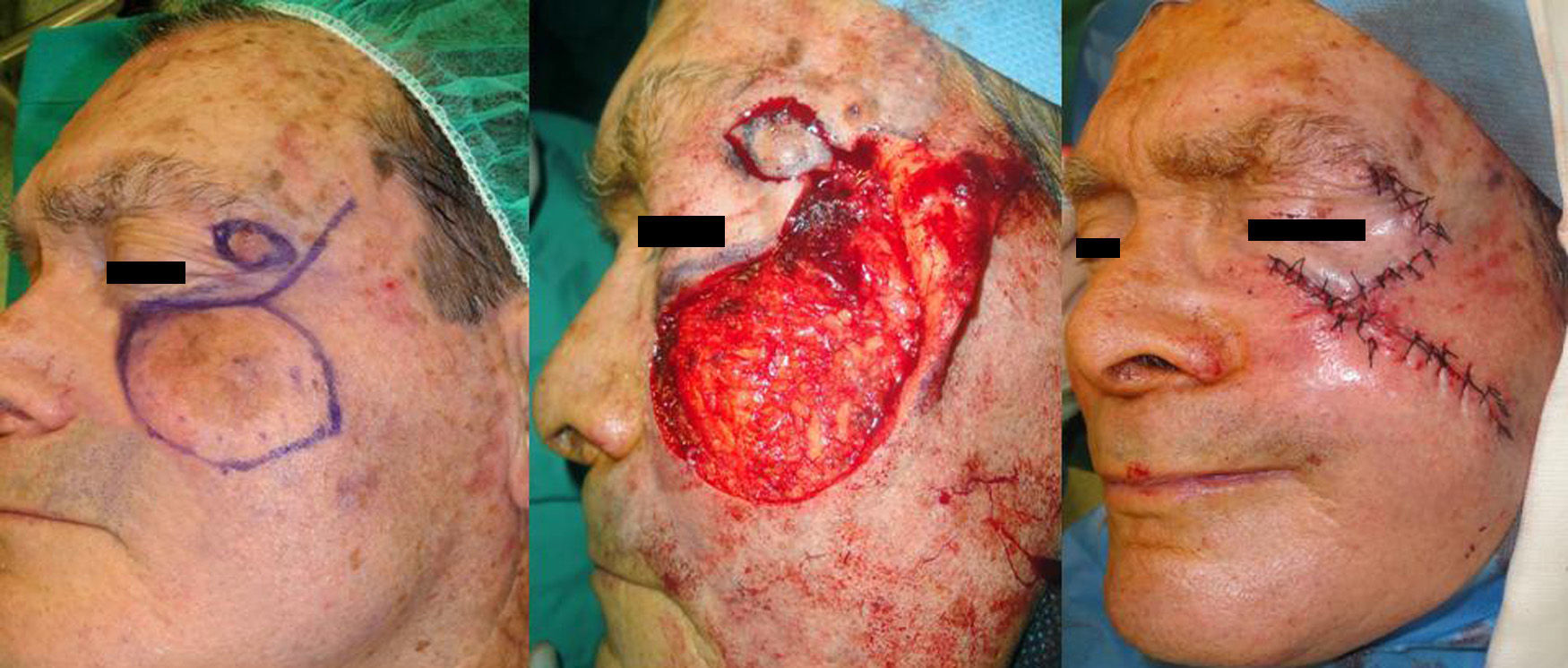
This patient was a 72-year-old man who presented a solid sclerodermiform basal cell carcinoma of 1×0.8cm in the malar region. After excision, an advancement-rotation flap was designed, respecting the tension lines of the cheek. The inferior part of the defect was triangulated and a semicircle of healthy skin was excised along the superolateral border to facilitate positioning of the flap. The borders of the flap were sutured with 4/0 silk (Fig. 3).
Case 4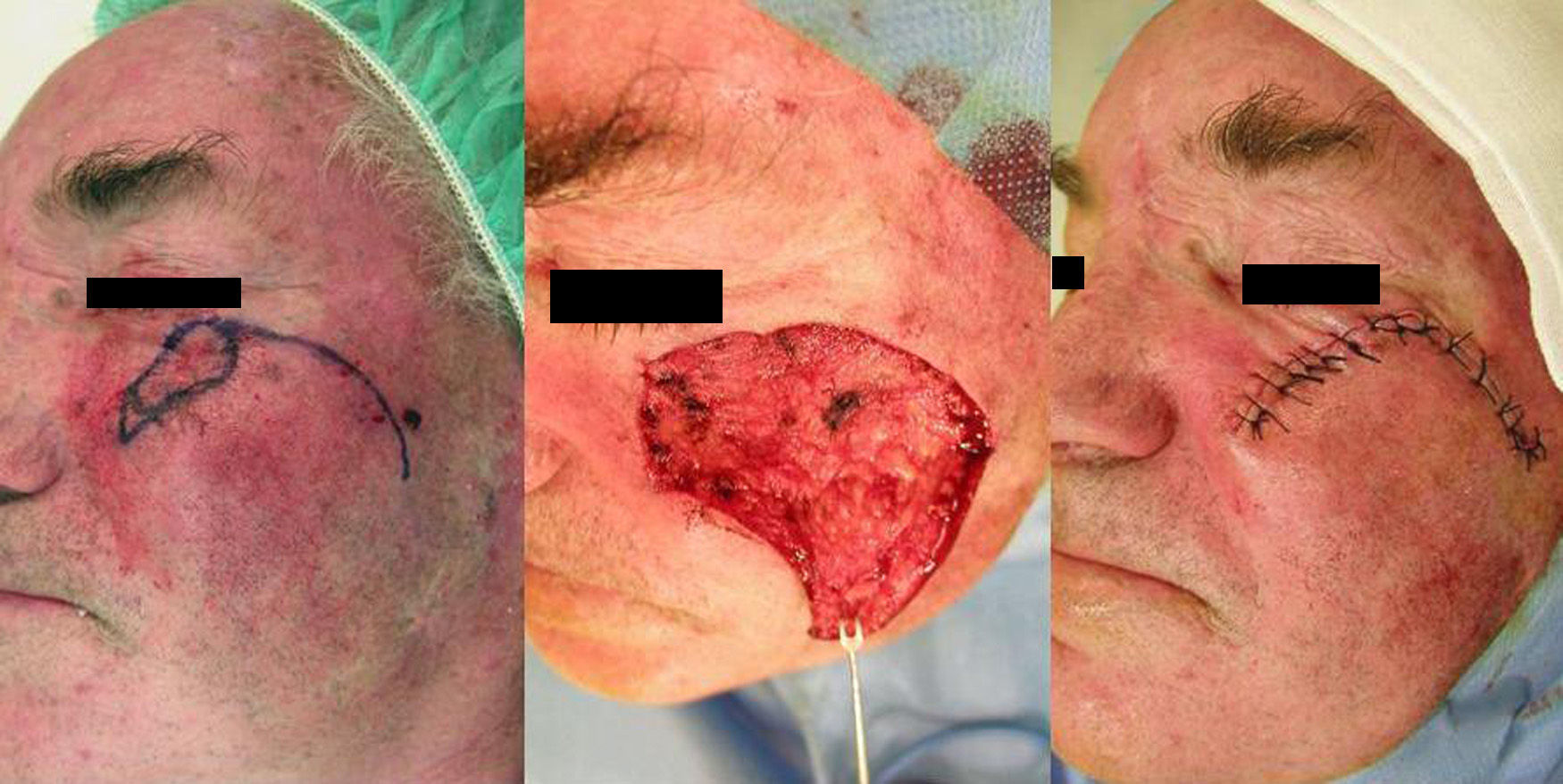
This patient was a man aged 77 years with a basosquamous carcinoma of 4.5×2.5cm in the area of the right lateral canthus and right malar region. After excision of the lesion, the defect was covered by a transposition flap taken from the frontotemporal region, above the ipsilateral eyebrow. The skin was sutured with 4/0 and 5/0 silk (Fig. 4).
Case 5
A 79-year-old man presented a lentigo maligna with a diameter of approximately 2.5cm situated on the lateral half of the right palpebromalar region. The surgical defect left by the excision was closed using a Limberg flap from the temporal region (Fig. 5). The skin was sutured with 4/0 silk.

Good clinical, functional, and cosmetic outcomes were achieved in all the cases presented.
DiscussionThe choice of surgical technique will depend on the site, size, thickness, and histological characteristics of the tumor. We must also take into account the age and general state of health of the patient.3 The main objective, as in any oncologic surgery, is radical excision of the tumor; prevention of the distortion of local structures and achieving the best cosmetic outcome are secondary objectives. To obtain the best cosmetic outcome, we must locate the donor site with the greatest tissue reserve and choose the best reconstruction technique. This is important in the medial zygomatic area, where an inappropriate choice can lead to ectropion and a very visible scar.1
A number of reconstruction techniques are available for use at this site. Whenever size permits, primary closure should be chosen. Second-intention healing is not to be recommended, as scar retraction will lead to ectropion. Grafts enable us to cover large defects, but apart from the typically poor cosmetic result in this region, graft retraction can lead to deformities of the adjacent facial subunits.2
In our first case, with a medium-sized tumor, the largest tissue reservoir was in the lateral subunit. We decided to use an advancement-rotation flap from the cheek that required a Z-plasty in the preauricular region to allow greater movement. If further tissue mobilization had been necessary, we could have prolonged the zygomatic incision along the preauricular sulcus, even onto the neck.2 Belmahi et al.4 described a flap that combined the classic Mustardé flap with a temporoparietal rotation flap that is used to cover the secondary defect left by the Mustardé flap. This technique can be used for defects of up to 7cm.5 Other, less desirable alternatives include use of the skin from the medial melolabial area or interpolation flaps.
In the second patient, the largest diameter of the surgical defect ran obliquely. The main tissue reservoirs were in the temporal, lateral, and medial buccal subunits. We could therefore have created a preauricular or melolabial advancement-rotation flap or a combination of the two. The existence of a second tumor on the upper eyelid and our evaluation of the elasticity of the skin led us to choose an advancement flap from the temporal subunit. The excision of the tumor on the eyelid served as a tension-relieving triangle for mobilization of the flap.6
The third patient presented a small tumor. Primary suture would have been the treatment of choice, but the patient's skin was difficult to mobilize, which would have led to a high risk of ectropion. The main skin reservoirs were in the zygomatic and upper medial subunits. We decided to use a rotation-advancement plasty from the cheek, following the skin tension lines. A medial plasty would have required incision of the eyelid, which often provokes persistent edema.
The tumor in the fourth patient, in contact with the lateral canthus, affected part of both eyelids and the cheek. The main skin reservoirs were the lateral cheek and the temporal region. We rejected the lateral cheek option because the skin is hairy. Instead we chose a supraciliary transposition flap.7
The final patient presented a smaller lesion than the previous patient, but it was at a similar site and the decisions were therefore very similar. The possible tissue reservoirs were the upper medial and the temporal subunits. From the medial area we could fashion a transposition flap with a superior base or a rotation flap with an incision along the melolabial fold. In the temporal region we could use transposition plasties, as above, or a Limberg flap. This patient had sufficient skin in the temporal region and even more close to the lateral canthus, and we thus considered a rhomboidal flap to be a good choice.
It may sometimes be necessary to use combinations of flaps to repair defects in this area.8,9
The main disadvantage of advancement-rotation plasties in the medial zygomatic region of the cheek (cases 1, 2, and3) is the risk of postsurgical ectropion if the flap is not correctly designed. The major complication of transposition flaps (cases 4 and5), on the other hand, is displacement of the lateral canthus.
When the tension vectors are vertical or horizontal, it may be necessary to anchor the flap to the periostium of the orbital rim to avoid traction on the lower eyelid.10
Reconstruction of the medial zygomatic subunit, one of the subunits of the cheek, is particularly complicated. We have described 5 possible reconstruction techniques for this area, discussing other alternatives and explaining the reasons for which we chose each of the options used.
Ethical DisclosuresProtection of human and animal subjects.The authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they followed their hospital's regulations regarding the publication of patient information and that written informed consent for voluntary participation was obtained for all patients.
Right to privacy and informed consentThe authors declare that no private patient data are disclosed in this article.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Pérez-Paredes M, González-Sixto B, Otero-Rivas MM, Rodríguez-Prieto MA. Cirugía reconstructiva de la región cigomática-medial de la mejilla: Presentación de 5 casos. Actas Dermosifiliogr. 2014;105:e27–e31.


