







Iso-Kikuchi syndrome, or congenital onychodysplasia of the index finger, is an uncommon condition characterized by total anonychia or dysplasia of the nail of the index finger. It is occasionally accompanied by underlying bone abnormalities and is rarely associated with other conditions. Although various hypotheses have been put forward to explain the pathophysiology of the syndrome, its etiology remains unknown.
We report the cases of 3 pediatric patients (2 boys and 1 girl) with nail changes and bone abnormalities consistent with Iso-Kikuchi syndrome. We highlight the importance of recognizing this entity early to avoid the need for additional tests and unnecessary treatment.
El síndrome de Iso-Kikuchi, onicodisplasia congénita del dedo índice, es una entidad poco frecuente caracterizada por la anoniquia total o displasia de la uña del dedo índice, acompañado, en algunas ocasiones, de alteraciones óseas subyacentes, por lo general, en ausencia de otras anomalías. Si bien se han planteado distintas hipótesis fisiopatogénicas, la etiología sigue siendo desconocida.
Describimos los casos de 3 pacientes pediátricos, 2 varones y una niña, con alteraciones ungueales y óseas compatibles con el síndrome de Iso-Kikuchi. Destacamos la importancia de reconocer esta entidad tempranamente para evitar la realización de estudios complementarios y terapéuticas innecesarias.
Iso-Kikuchi syndrome is characterized by anonychia or onychodysplasia of the index finger, accompanied or not by underlying bone abnormalities. It is a benign condition that is not associated with alterations to other organs or systems. Very few cases have been reported to date.
Case DescriptionsTwo boys and 1 girl presented with Iso-Kikuchi syndrome for the first time between the ages of 2 and 4 years.
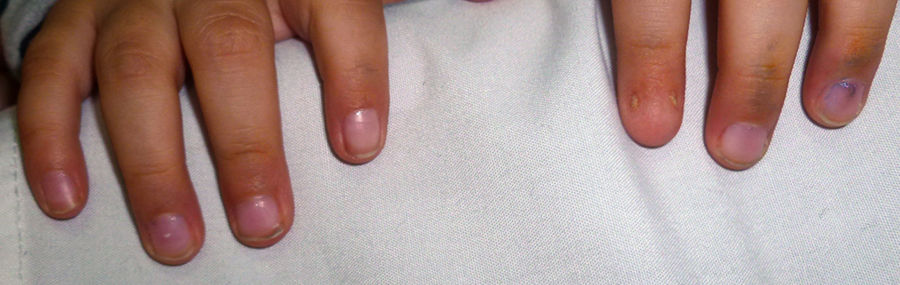
Patient #1, a 2-year-old boy, had bilateral index finger involvement and a Y-shaped deformity of the underlying phalanx (Fig. 1). His past medical history was remarkable for extreme preterm birth (30 weeks), which is why we have included other diseases associated with this condition in Table 1.

Cases Presented.
| Patient | 1 | 2 | 3 |
|---|---|---|---|
| Sex | Male | Female | Male |
| Age | 2 y | 4 y | 2 y |
| Perinatal history | Born at 30 wk; nail changes present at birth | Term delivery; nail changes present at birth | Term delivery; nail changes present at birth |
| Digit involved | Both index fingers | Left index finger | Both index fingers |
| Appearance of other nail | Micronychia on radial side | Micronychia on radial and ulnar sides | One finger with polyonychia, dystrophic homolateral finger |
| Radiographic changes | Bilateral Y-shaped deformity | Y-shaped deformity in affected finger | None |
| Other alterations | Grade 3 intraventricular hemorrhage, bilateral inguinal bleeding, bilateral pelviureteric junction stenosis | None | Gastroesophageal reflux |
| Family history | No | No | No |
Patient #2, a 4-year-old girl, had involvement of the left index finger and a Y-shaped bifurcation of the affected phalanx (Fig. 2).
Patient #3 was 2 years old and had bilateral index finger involvement (Fig. 3) without radiographic changes (Table 1).

None of the patients’ relatives had Iso-Kikuchi syndrome. All the parents denied consanguinity and reported that their children's nail alterations had been present since birth.
DiscussionIso-Kikuchi syndrome was first described by Dr. Iso in 1969 and Dr. Kikuchi in 1974,1–3 and very few cases have been reported since (Table 2). It affects both sexes equally and can be sporadic or familial.
Cases Published in the Literature.
| Publication | Reference | No. of Patients | Age | Sex | Characteristics | Other |
|---|---|---|---|---|---|---|
| Di Chiacchio et al. | 3 | 1 | 13 y | Not specified | Micronychia and altered lunula of right index finger Micronychia, malalignment, and irregular lunula of left index finger | No |
| Valerio et al. | 4 | 1 | Neonate | Not specified | Complete anonychia of left middle finger | Mother: consumption of mebendazole during pregnancy |
| Baran & Stroud | 5 | 1 | 41 y | Male | Hemionychogryphosis of right and left index fingers and abnormal lunula | No |
| Hussein et al. | 7 | 1 | 52 y | Female | Ulnar micronychia of both index fingers | Leukonychia of both hands |
| Thappa & Shivaswamy | 8 | 1 | 20 y | Male | Polyonychia of right index finger | No |
| Iso | 1 | |||||
| Kikuchi et al. | 2 | 2 | 5 y 29 y | Female Female | Polyonychia of right and left index fingers and absent lunulae Polyonychia of left index finger; hemionychogryphosis of contralateral nail | Radiography: narrowing of distal phalanx of both index fingers, brachymesophalangy of thumbs Radiography: brachymesophalangy of both thumbs |
| Kikuchi et al. | 6 | 2 | 24 y 4 mo | Female Female | Ulnar micronychia of both index fingers Polyonychia of left index finger | Radiography: Y-shaped bifurcation Radiography: hypoplasia of underlying phalanx |
Iso-Kikuchi syndrome runs an indolent course that is characterized by anonychia or onychodysplasia of the index finger possibly accompanied by bone abnormalities in the underlying phalanx.4 It can affect one or both hands or feet. Based on their observations and analysis of different clinical cases, Baran and Stroud5 proposed the following diagnostic criteria for Iso-Kikuchi syndrome: 1) unilateral or bilateral hypoplasia (up to complete anonychia) of the index finger and/or other fingers or toes, 2) radiographic changes in the distal phalanx of the affected digit; and 3) sporadic or hereditary congenital occurrence. Transmission of Iso-Kikuchi syndrome is autosomal dominant. No associations with systemic diseases have been reported.4,5
Onychodysplasia has multiple presentations (Table 2), the most common of which are anonychia, micronychia (characteristic deviation of the nail to the ulnar side of the nail bed),6polyonychia (2 nails, 1 on each side of the nail bed), hemionychogryphosis, irregular lunula, and nail malalignment.
Narrowing of the distal phalanx is a characteristic radiographic finding, but it is not always present. This narrowing will be seen on anteroposterior radiographs, whereas lateral projections will show the corresponding Y-shaped bifurcation.3–8 Other, less common, bone changes include brachydactyly, brachymesophalangia, and brachymetacarpia.7,8
The etiologic and pathogenic mechanisms of Iso-Kikuchi syndrome are not fully understood, and while several theories have been put forward, none of them have been fully accepted. Notable causes are mutations in the Wnt signaling pathway during embryogenesis, in utero damage to arterioles that depend on the radial artery (which has a smaller diameter than the ulnar artery), osteodystrophy of the phalanx during embryogenesis, and consumption of teratogenic drugs (anticonvulsants) during pregnancy.4
Diagnosis is mostly clinical. Iso-Kikuchi syndrome should be suspected in patients with congenital nail changes affecting one or both index fingers in the absence of other hand alterations, particularly when characteristic radiographic alterations are observed. The differential diagnosis should include other congenital nail changes, such as ectodermal dysplasia, pachyonychia congenita, nail-patella syndrome, and deafness-onychodystrophy syndrome. Although nail changes are present from an early age in all these diseases, they have distinctive clinical characteristics and are often accompanied by extracutaneous alterations. The differential diagnosis may also include acquired nail changes due to trauma or infection, but these can be distinguished by their postnatal onset.
Iso-Kikuchi syndrome is a rare, benign syndrome with characteristic clinical features. We have presented 3 new pediatric cases and highlight the importance of early recognition to avoid the need for unnecessary tests and treatment.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
We thank Bruno Mentasti for his help with editing the photographs.
Please cite this article as: Tirelli LL, Luna PC, Cano R, Giraldo JP, Larralde M. Síndrome de Iso-Kikuchi: 3 casos en la edad pediátrica. Actas Dermosifiliogr. 2018;109:e33–e36.


