
There is strong evidence that psoriasis is associated with several cardiometabolic comorbidities, and that patients with psoriasis are at a higher risk of cardiovascular morbidity and mortality.1–3 Understanding this is of crucial importance, not only for physicians but also for patients, as it can impact prognosis and patient quality of life.4
It has been shown that few patients with moderate to severe psoriasis are aware of their increased risk of atherothrombotic disease and metabolic syndrome.5 Educational sessions are a recognized tool for informing and helping patients to understand the nature and course of their disease and the different treatments available, and can also help them to develop coping strategies.6,7
We performed an observational study to evaluate the impact of an educational session designed to promote knowledge among patients with psoriasis about their disease, lifestyle changes, and management of cardiometabolic comorbidities.
The educational session was held in the psoriasis unit of a Portuguese tertiary hospital. Briefly, it consisted of several oral presentations (30min each) explaining the nature of psoriasis, introducing the various treatment options, exploring the association between psoriasis and cardiometabolic comorbidities/cardiovascular disease, and underlining the importance of monitoring and treating these. A questionnaire was created for the patients to complete before, immediately after, and 6 months after the session. The questionnaire included demographic information, questions regarding the association between psoriasis and cardiometabolic comorbidities/cardiovascular disease, and assessment of lifestyle and comorbidity management.
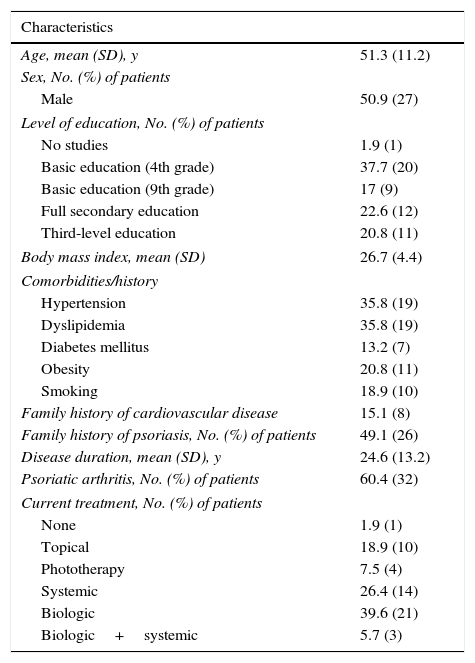
Seventy patients participated in the session and 53 completed all 3 questionnaires correctly. The demographic data, characteristics of disease, and treatments received are presented in Table 1. Regarding cardiometabolic comorbidities, 35.8%, 13.2%, and 35.8% of patients had a respective diagnosis of hypertension, diabetes mellitus, and dyslipidemia; 20.8% were obese (body mass index>30); and 18.9% were active smokers (Table 1).
Characteristics of 53 patients who completed full questionnaires before and after a psoriasis education session.
| Characteristics | |
|---|---|
| Age, mean (SD), y | 51.3 (11.2) |
| Sex, No. (%) of patients | |
| Male | 50.9 (27) |
| Level of education, No. (%) of patients | |
| No studies | 1.9 (1) |
| Basic education (4th grade) | 37.7 (20) |
| Basic education (9th grade) | 17 (9) |
| Full secondary education | 22.6 (12) |
| Third-level education | 20.8 (11) |
| Body mass index, mean (SD) | 26.7 (4.4) |
| Comorbidities/history | |
| Hypertension | 35.8 (19) |
| Dyslipidemia | 35.8 (19) |
| Diabetes mellitus | 13.2 (7) |
| Obesity | 20.8 (11) |
| Smoking | 18.9 (10) |
| Family history of cardiovascular disease | 15.1 (8) |
| Family history of psoriasis, No. (%) of patients | 49.1 (26) |
| Disease duration, mean (SD), y | 24.6 (13.2) |
| Psoriatic arthritis, No. (%) of patients | 60.4 (32) |
| Current treatment, No. (%) of patients | |
| None | 1.9 (1) |
| Topical | 18.9 (10) |
| Phototherapy | 7.5 (4) |
| Systemic | 26.4 (14) |
| Biologic | 39.6 (21) |
| Biologic+systemic | 5.7 (3) |
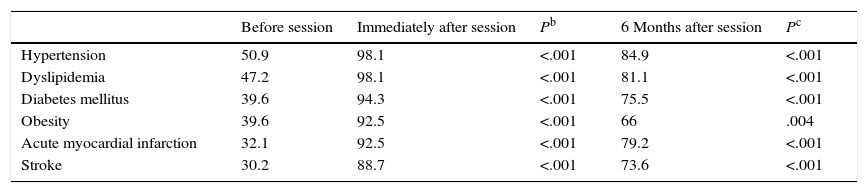
The McNemar test was used to assess significant improvements in knowledge between the different time points. A P value of less than or equal to .05 was considered statistically significant. A significant increase was observed in the percentage of correctly answered questions about the association between psoriasis and cardiometabolic comorbidities/cardiovascular disease on comparing the answers before and immediately after the session and before the session and 6 months later (Table 2). When logistic regression models adjusting for age, sex, and level of education were applied, the results were not altered.
Improvements in awareness of association between psoriasis and cardiometabolic comorbidities/cardiovascular disease.a
| Before session | Immediately after session | Pb | 6 Months after session | Pc | |
|---|---|---|---|---|---|
| Hypertension | 50.9 | 98.1 | <.001 | 84.9 | <.001 |
| Dyslipidemia | 47.2 | 98.1 | <.001 | 81.1 | <.001 |
| Diabetes mellitus | 39.6 | 94.3 | <.001 | 75.5 | <.001 |
| Obesity | 39.6 | 92.5 | <.001 | 66 | .004 |
| Acute myocardial infarction | 32.1 | 92.5 | <.001 | 79.2 | <.001 |
| Stroke | 30.2 | 88.7 | <.001 | 73.6 | <.001 |
Six months after the session, 60.4% of respondents stated that they had started to exercise or had increased their level of physical activity; 49.1% stated that they had lost weight (mean loss, 2.3kg; maximum loss, 7kg; minimum loss, 1kg); and 50% stated that they had cut down on smoking, although none had quit.
After the session, over 90% of the participants stated that they were willing to consult their general practitioner to screen for cardiometabolic comorbidities or monitor those already diagnosed. This attitude led to newly diagnosed comorbidities (7 cases of dyslipidemia, 2 cases of hypertension, and 2 cases of diabetes mellitus) and therapeutic adjustments (in 4 cases of hypertension, 4 cases of dyslipidemia, and 1 case of diabetes mellitus).
Our results show that an educational session held with patients with psoriasis had a real impact on their health, leading to lifestyle changes (physical activity, weight loss, reduction of smoking), increased awareness of their disease and associated comorbidities, and new diagnoses of cardiovascular risk factors or therapeutic adjustments. Repeated educational sessions with the same group of patients might further improve these positive results.
Some limitations of this study must, however, be mentioned, mainly the limited number of participants and a potential response bias, either intentional or due to comprehension factors, associated with self-reported surveys.
In brief, this educational intervention proved to be a useful tool that had significant repercussions on patients’ health, life, and ability to cope with the disease, and it should therefore be repeated with a larger number of patients.
Conflict of interestThe authors declare no conflict of interest.


