


Port wine stain (PWS) is a type of capillary malformation than can be disfiguring. Although diagnosis is based on clinical findings,1 the availability of an objective method for evaluating the density and depth of the vessels can help to predict the response to treatment and monitor the stains.2 Therefore, we designed a pilot study with 2 objectives: (1) to compare the ultrasound characteristics of skin with PWS using high-sensitivity Doppler for the detection of slow-flow vessels (X flow) and contralateral healthy skin; (2) to evaluate whether the blood vessels in PWS can be better visualized with X flow than with conventional Doppler.
We included 20 patients with PWS (10 men and 10 women) who were evaluated in 2015. Sixteen of the 20 patients had previously received treatment with pulsed-dye laser (MultiPlex R, Cynergy) (Table 1). The affected skin and the healthy contralateral skin were evaluated using conventional Doppler ultrasound and X flow. We used an ultrasound device with a 22-MHz transducer (MyLab, Esaote). The images were reviewed by 2 blinded observers, who reported which of the images revealed greater vessel density, with both conventional Doppler and X flow. Clinical and ultrasound images were also recorded (Fig. 1).
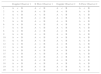
Patient Characteristics.
| Sex | Age, y | Location | Previous Treatment With PDL |
|---|---|---|---|
| Female | 22 | Left cheek | 5 |
| Female | 38 | Nasal dorsum | 6 |
| Male | 55 | Upper back | 1 |
| Male | 43 | Left forehead | 4 |
| Male | 43 | Left neck | 0 |
| Male | 47 | Left hip | 4 |
| Male | 54 | Right cheek | 0 |
| Male | 52 | Left V2 | 0 |
| Female | 25 | Right leg | 3 |
| Male | 38 | Left V3 | 0 |
| Male | 51 | Scalp | 0 |
| Male | 7 | Left leg | 0 |
| Female | 46 | Left V2 | 3 |
| Female | 57 | Left V2 | 3 |
| Female | 42 | Left V2 | 3 |
| Female | 38 | Right V2 | 1 |
| Female | 24 | Left V3 | 1 |
| Female | 14 | Left hand | 1 |
| Female | 52 | Right V2 | 1 |
| Male | 57 | Left chest | 1 |
Abbreviation: PDL, pulsed-dye laser.

The results are summarized in Table 2. Observer 1 reported greater Doppler flow in the PWS than in the healthy skin in 40% of cases and equal Doppler flow in 55%. X flow mode revealed greater flow in the PWS than in healthy skin in 15 patients (75%) and equal flow in 5 (25%), with no cases of greater flow in healthy skin than in affected skin (0%). Observer 2 reported similar findings, namely, greater Doppler flow in the PWS than in healthy skin in 8 cases (40%) and equal flow in 12 cases (60%). X flow mode revealed flow to be greater in the PWS than in healthy skin in 15 patients (75%) and equal in 5 (25%), with no evidence of greater flow in healthy skin than in affected skin (0%).
Results.
| Doppler Observer 1 | X Flow Observer 1 | Doppler Observer 2 | X Flow Observer 2 | |
|---|---|---|---|---|
| 1 | A<B | A<B | A<B | A<B |
| 2 | A<B | A<B | A<B | A<B |
| 3 | A<B | A<B | A<B | A<B |
| 4 | A=B | A<B | A=B | A=B |
| 5 | A=B | A=B | A=B | A=B |
| 6 | A<B | A<B | A<B | A<B |
| 7 | A<B | A<B | A<B | A<B |
| 8 | A<B | A<B | A<B | A<B |
| 9 | A=B | A=B | A=B | A<B |
| 10 | A=B | A<B | A=B | A<B |
| 11 | A<B | A<B | A<B | A<B |
| 12 | A=B | A=B | A=B | A=B |
| 13 | A=B | A<B | A=B | A<B |
| 14 | A=B | A<B | A=B | A<B |
| 15 | A=B | A<B | A=B | A<B |
| 16 | A<B | A<B | A<B | A<B |
| 17 | A=B | A<B | A=B | A<B |
| 18 | A=B | A<B | A=B | A<B |
| 19 | A>B | A=B | A=B | A=B |
| 20 | A=B | A=B | A=B | A=B |
Abbreviations: A, healthy skin; B, port wine stain.
At present, the treatment of choice for PWS is pulsed-dye laser, which enables the lesion to be treated without damaging the surrounding tissue.1 However, the results are not satisfactory: complete resolution is achieved in only 10% of cases, and 20%-30% of cases are completely refractory.2
Very few studies have assessed PSW using ultrasound. Troilus et al.3 analyzed 55 cases in which ultrasound was used to assess the depth of the PWS and to establish an association with response to pulsed-dye laser treatment. This is of interest, since the penetration of pulsed-dye laser ranges from 0.65mm according to Hohenleutner et al.2 to 1.2mm according to Tan et al.4 Therefore, the thickness of the PWS and the depth and diameter of the vessels play a key role in the response to treatment.
Ultrasound is a noninvasive method of obtaining objective information on PWS. B mode reveals hypoechogenicity in the dermis, which is more evident in thicker PWS, although this should not be confused with solar elastosis (which requires monitoring of healthy skin). With color Doppler, we find increased vascularization in the dermis; pulsed Doppler reveals neither veins nor arteries.5 Of note, Troilus et al.3 reported that a high percentage of PWS (10%) are not visible using ultrasound; in our experience, this percentage could be even higher (20%).
Modes such as X flow (Esaote, MyLab) and B mode (General Electric) enable real-time evaluation of red cells that move within the vascular lumen. The display is obtained by transmitting digitally coded broadband pulses, which are reflected by mobile cells. The echoes that return are decoded and filtered, thus amplifying the weak echoes of the blood cells and eliminating or attenuating echoes in the surrounding tissue. These methods are visual—not quantitative—and make it possible to detect smaller or low-flow vessels. In addition, one of their advantages is the reduced dependency on the angle and the ability to work in real time more dynamically than with conventional Doppler.
A notable limitation is the fact that most patients had previously received laser treatment. It would therefore be interesting to perform a prospective study to compare X flow images before and after treatment as a complement to clinical observation.
The present study revealed considerable agreement between the 2 observers, which in the case of X flow was 100%. Therefore, we believe that X flow mode provides a better evaluation of PWS, since it is more efficacious for detecting small-caliber, low-flow vessels.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Salgüero Fernández I, Alfageme Roldán F, Roustan Gullón G. Superioridad en la detección de vasos de pequeño calibre con modo X flow frente al doppler convencional en la mancha en vino de Oporto. Estudio piloto. Actas Dermosifiliogr. 2017;108:690–692.


