


An 89-year-old woman, with a past history of systemic hypertension, aortic stenosis, and iron deficiency anemia and on treatment with hydrochlorothiazide, lisinopril, and acetylsalicylic acid, was seen for an asymptomatic lesion that had arisen a month earlier in her left frontoparietal region. She had been treated with topical corticosteroids, which were prescribed for suspected contact eczema to hair dye. Physical examination revealed an erythematous-violaceous plaque that extended down to her cheek. The surface of the lesion presented a small nodule of vascular appearance (Fig. 1, A and B).

A, Erythematous-violaceous plaque with well-defined borders in the frontotemporal region. B, Proliferation of neoplastic endothelial cells with nuclear hyperchromatism and nucleomegaly, forming vascular spaces that dissect between the collagen bundles in the dermis. Hematoxylin and eosin, original magnification,x10.
B-mode ultrasound (18MHz probe, eSaote, MyLab25Gold) showed a predominantly hypoechoic nodule of 3.7mm×16.5mm with well-defined borders, situated in the deep dermis and subcutaneous cellular tissue (Fig. 2A). The periphery of the lesion presented mixed echogenicity, in contrast to the more hypoechoic central area. In the deep region of the lesions was a hyperechoic area that may have been posterior enhancement. The epidermis appeared as a hyperechoic band. The lesion extended diffusely peripherally, and it was more difficult to identify its borders in this plane (Fig. 2, B andC). At the lateral borders of the lesion and in the non-nodular part of the tumor, areas of mixed echogenicity predominated over the hypoechoic areas. Color Doppler showed an irregular asymmetric neovascularization at the periphery of the lesion (Fig. 2, B andC).

A, Hypoechoic nodule with well-defined borders that are slightly more echogenic than the center of the nodule. B, Color Doppler showed increased vascularity and asymmetrically distributed medium-sized vessels in the base of the nodule. C, Increased vascularity in the non-nodular area of the lesion.
Histology performed on an ultrasound-guided punch biopsy revealed a poorly defined neoplastic proliferation in the dermis, forming of anastomosing vascular spaces growing between the collagen bundles and skin appendages; the spaces were lined by endothelial cells with nuclear hyperchromatism and nucleomegaly, with frequent pleomorphic nuclei (Fig. 1B). Stain for human herpesvirus 8 was negative. Based on the clinical, ultrasound, and histopathological findings, we made a diagnosis of idiopathic angiosarcoma of the head and neck.
Idiopathic angiosarcoma of the head and neck is a rare neoplasm first described by Caro and Stubenrauch in 1945. It is formed of proliferations of cells with endothelial differentiation. The lesions initially appear as erythematous plaques that rapidly progress to violaceous nodules that bleed easily. This type of angiosarcoma grows centrifugally, and can occupy large areas of the face and neck.1 The clinical differential diagnosis should include entities such as rosacea,2,3 lymphoma, skin metastases, pyogenic granuloma, and Kaposi sarcoma. The prognosis is poor, with a 5-year survival of less than 15%.4,5 Surgical excision, when possible, is the treatment of choice. Chemotherapy with taxanes and palliative radiotherapy are second line treatment.6 Because of our patient's advanced age and the size of the lesion, it was decided to start treatment with weekly paclitaxel at a dose of 60mg/m2, with a poor response.
Cutaneous angiosarcoma presents histologically as a poorly defined dermal tumor with vascular tracts that infiltrate the dermis and subcutaneous cellular tissue. The endothelium can be several layers thick and contain mitotic cells. The tumor usually dissects between the collagen fibers. Ultrasound reveals hypoechoic nodules with a mixed peripheral echogenicity. The lower echogenicity of the center of the nodules may correlate with greater tumor mass and cellularity in this central region, characteristic of neoformation. The mixed peripheral echogenicity may indicate reduced cellularity in this peripheral area and dissection of the collagen bundles by tumor cells.
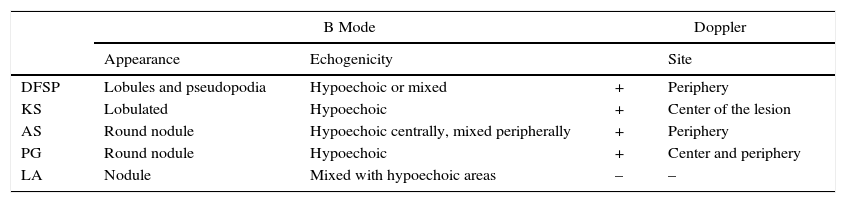
Ultrasound enables us to clarify the differential diagnosis with certain other conditions, such as dermatofibrosarcoma protuberans, which is characterized by lesions with distinct echogenicity and a lobulated appearance with pseudopodia, and a weak Doppler signal peripherally.7 Kaposi sarcoma is seen as a hypoechoic lesion with an increased Doppler signal within the lesion, in contrast to angiosarcoma, in which the Doppler signal is increased peripherally.7,8 Pyogenic granuloma presents as a well-defined, oval hypoechoic lesion in the dermis and subcutaneous cellular tissue, with low-flow central and peripheral vascularity on Doppler study.7 Lymphangiomas are poorly vascular lesions, and this is evident on ultrasound.8 Angiosarcoma of the breast has been reported to present hypoechoic images in the dermis and in the subcutaneous cellular tissue, with a contour showing lobules and spicules8 (Table 1).
Ultrasound Characteristics of the Main Conditions to be Included in the Differential Diagnosis.
| B Mode | Doppler | |||
|---|---|---|---|---|
| Appearance | Echogenicity | Site | ||
| DFSP | Lobules and pseudopodia | Hypoechoic or mixed | + | Periphery |
| KS | Lobulated | Hypoechoic | + | Center of the lesion |
| AS | Round nodule | Hypoechoic centrally, mixed peripherally | + | Periphery |
| PG | Round nodule | Hypoechoic | + | Center and periphery |
| LA | Nodule | Mixed with hypoechoic areas | – | – |
Abbreviations: AS, angiosarcoma; DFSP, dermatofibrosarcoma protuberans; KS, Kaposi sarcoma; LA, lymphangioma; PG, pyogenic granuloma.
In the literature reviewed, we found no reports that describe the ultrasound characteristics of idiopathic angiosarcoma of the head and neck; the only available descriptions are of angiosarcoma of the breast.8 In this first description of the ultrasound findings in cutaneous angiosarcoma of the head and neck, ultrasound made guided skin biopsy possible, improving the yield and avoiding the possible complications of blind biopsy. When surgical excision is a therapeutic option, ultrasound could be an interesting tool to help define the borders of the lesion.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Boas PV, Martínez AR, Rodriguez OB, Blanco CC. Primera descripción ecográfica del angiosarcoma cutáneo idiopático de cabeza y cuello. Actas Dermosifiliogr. 2017;108:960–962.


