





Circumscribed palmoplantar hypokeratosis (CPH) is a rare disease characterized by focal thinning of the stratum corneum. It manifests as a round, well-defined, depressed, erythematous lesion with a scaly border, generally located on the palms. It is generally asymptomatic and predominantly affects middle-aged or elderly women. We report 3 cases of CPH on the sole of the foot, a rare site for this disease.
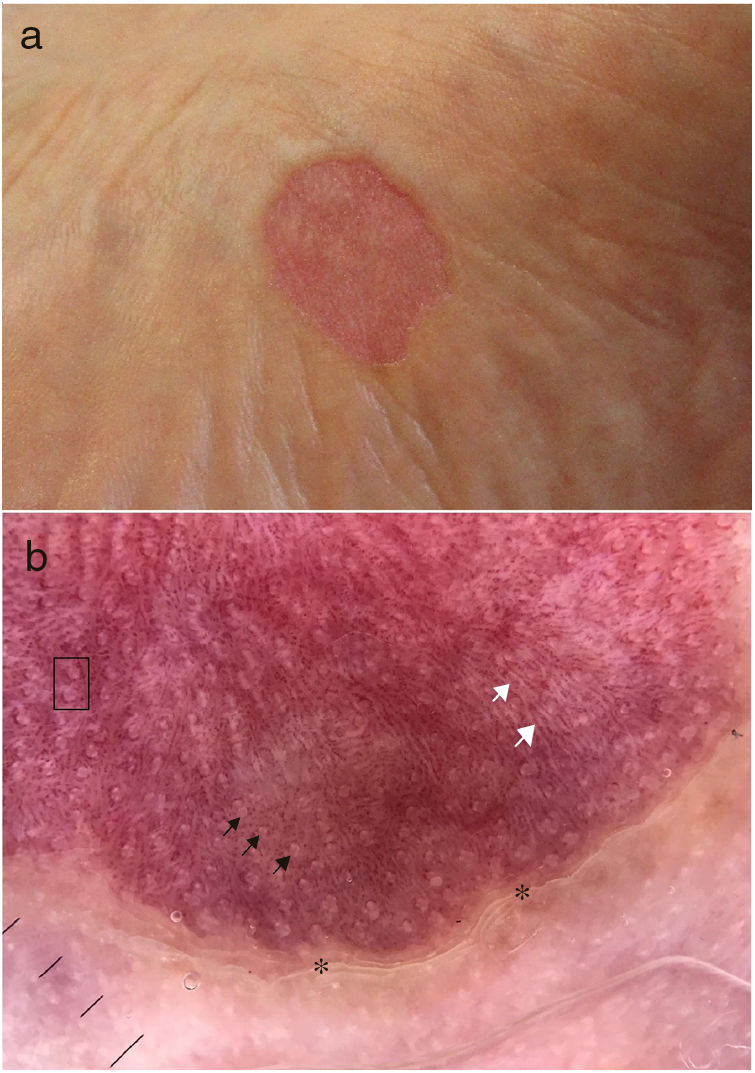
Case 1. A 74-year-old diabetic man who visited our department with an asymptomatic erythematous lesion on the sole of the left foot; the lesion had well defined borders and had grown slowly over the previous 7years (Fig. 1A) . Dermatoscopy revealed a stepped scaly border, an erythematous base with punctate vessels, regular white spots occasionally surrounded by the punctate vessels, and thin white lines (Fig. 1B). Clinical and dermatoscopic data were compatible with CPH. The patient refused a biopsy and did not want to undergo treatment.
Case 2. An 82-year-old woman with no relevant past history visited our department with a mildly pruritic lesion on the inside surface of the right foot that had grown slowly over the previous 4years. Physical examination revealed a lesion measuring 12×10mm with well-defined borders and a depressed erythematous center. Dermatoscopy revealed similar findings to the previous case. The biopsy showed a sudden reduction in the thickness of the stratum corneum, with hypergranulosis and diffuse areas of parakeratosis with no evidence of a parakeratotic column. CPH was diagnosed and the patient was treated with betamethasone dipropionate and calcipotriol, which produced a slight improvement. Treatment was suspended after a few weeks owing to irritation. The patient refused other treatments.
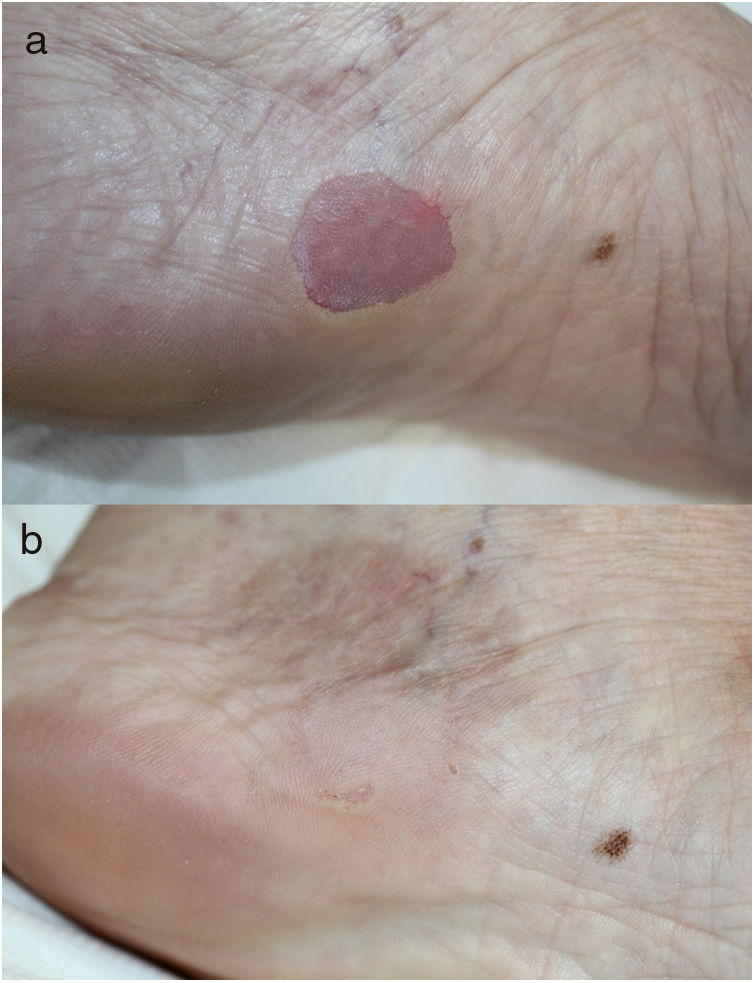
Case 3 A 69-year-old woman with no relevant past history visited our department with an asymptomatic, erythematous, depressed lesion on the arch of the left foot, with scaly border, which had appeared 10years earlier (Fig. 2A) . The dermatoscopy and histology findings were similar to the previous cases, confirming the diagnosis of CPH. The patient was treated with tacrolimus ointment 0.1% for 4months with little improvement. Cryotherapy with liquid nitrogen was then used and the lesion resolved completely (Fig. 2B).
CPH is a benign entity of unknown etiology that was first described in 2002 by Pérez et al.1 It is thought to be due to an abnormal keratinocyte clone that does not differentiate into palmoplantar epidermis, leading to marked thinning of the stratum corneum in comparison to the surrounding normal skin.2 Most of the cases described had no past history of trauma.
CPH is a rare disease, with approximately 100 cases reported in the literature.3 More than 60% of these cases were located on the thenar prominence, on the palm or back of the hand, on the sole of the foot, and on the medial surface of the foot. These last 2 locations are rare and account for less than 15% of reported cases of CPH.3,4 A review of the literature found 16published case of CPH on the sole of the foot1,3,4 (Table 1).
Review of Cases of Circumscribed Plantar Hypokeratosis Published to Date, With Clinical Characteristics, Treatments Used, and Response to Treatment.
| No. | Authors and Date | Age | Sex | Sole | Treatments | Clinical Course |
|---|---|---|---|---|---|---|
| 1 | Pérez et al.,1 2002 | 68 | Female | Left | Several | No change |
| 2 | Rütten et al.,3 2004 | 64 | Female | Left | None | NI |
| 3 | Berk et al.,3 2007 | 75 | Female | Left | 5-fluorouracil topical | No change |
| Calcipotriol ointment | No change | |||||
| Clobetasol ointment | No change | |||||
| 4 | Berk et al.,3 2007 | 49 | Female | Left | Fluocinolone cream | No change |
| Excision | Complete resolution | |||||
| 5 | Barry et al.,3 2008 | 59 | Male | Right | NI | NI |
| 6 | Tanioka et al.,3 2009 | 62 | Male | Right | Topical corticosteroids | No change |
| Antibiotics | No change | |||||
| 7 | Cribier et al.,3 2009 | 65 | Male | Left | None | No change |
| 8 | Kanitakis et al.,3 2011 | 56 | Female | Right | NI | NI |
| 9 | Arbesman et al.,3 2012 | 10 | Male | Left | NI | NI |
| 10 | Santamarina-Albertos et al.,3 2013 | 2 | Male | Right | Calcipotriol topical | No change |
| 11 | Batalla et al.,3 2013 | 17 | Male | Right | Calcipotriol topical | Complete resolution |
| 12 | Mitkov et al.,3 2014 | 73 | Male | Right | Mometasone topical | No change |
| Tacrolimus topical | No change | |||||
| Pimecrolimus topical | No change | |||||
| 5-fluorouracil topical | No change | |||||
| Cryotherapy | No change | |||||
| 13 | Pinos-León et al.,3 2014 | 55 | Female | Left | Topical corticosteroids | No change |
| Topical antimycotics | No change | |||||
| 14 | Ramos-Garibay et al.,3 2016 | 69 | Female | Left | Calcipotriol topical | No change |
| 15 | Ramos-Garibay et al.,3 2016 | 71 | Female | Left | None | No change |
| 16 | Nazzaro et al.,4 2016 | 80 | Male | Left | NI | NI |
| 17 | Aranguren-López et al., 2018 | 74 | Male | Left | None | NI |
| 18 | Aranguren-López et al., 2018 | 82 | Female | Right | Topical betamethasone dipropionate and calcipotriol | Slight improvement |
| 19 | Aranguren-López et al., 2018 | 69 | Female | Left | Cryotherapy | Complete resolution |
Abbreviation: NI indicates not indicated.
The histopathology of CPH is characteristic and confirms the diagnosis.2 A sudden interruption can be observed between the normal dermis and that of the lesion, which shows marked hypokeratosis and mild hypogranulosis. No parakeratotic column can be seen at the periphery of the lesion. This differentiates the disease from porokeratosis of Mibelli, the most clinically similar entity, which must be included in the differential diagnosis.2,5
Dermatoscopy is very useful for diagnosing this dermatosis. Typical findings are peripheral stepped desquamation (corresponding to the abrupt limit between the normal and hypokeratotic epidermis), a uniform erythematous base with small punctate vessels (reflection of the congestive capillaries in the underlying dermis, which become more visible due to the epidermal thinning) and regularly distributed white spots (the pores of the acrosyringia).5 White lines on the erythematous base,5 have been recently described, which correspond to the epidermal folds. The only dermatoscopy of palmoplantar hypokeratosis on the sole of the foot published to date4 describes for the first time distribution of the punctate vessels around the acrosyringia. These recent findings were also observed in our patients.
No effective treatment for CPH exists. In some of the reported cases,6 and in one of our patients, cryotherapy achieved complete remission of the lesions. Topical calcipotriol and 5-fluorouracil have also proven effective in some cases.2
In conclusion, we report 3 cases of CPH on the sole of the foot, a rare site for this rare disease, which is probably underdiagnosed due to its asymptomatic nature. We describe the dermatoscopic characteristics of the entity, which are very useful for diagnosis, and highlight the white lines found in one of our patients, which have been reported recently. We also highlight the utility of cryotherapy, which produced complete remission of the lesion in 1 case.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Aranguren-López I, Vildósola-Esturo S, Arias-Camisón I, López-Pestaña A. Hipoqueratosis plantar circunscrita. Actas Dermosifiliogr. 2019;110:619–621.


