





Female androgenetic alopecia is one of the main causes of hair loss, and affects 50% of women in their lifetime.1 Alopecia and hirsutism as a manifestation of hyperandrogenism in postmenopausal women can have various causes, ranging from normal physiological changes to an ovarian or adrenal tumor. Recommended tests in any woman presenting with alopecia are a detailed clinical history, physical examination, general blood tests (including complete blood count and thyroid stimulating hormone and ferritin levels) and a hormone study with measurement of dehydroepiandrosterone sulfate and total and free testosterone levels.
We present the case of a 65-year-old woman who presented with a 1-year history of hair loss and black facial hair. There was no past history of alopecia, hirsutism, or hyperandrogenism. Her history was remarkable for cardiovascular risk factors (hypertension, dyslipidemia, and diabetes mellitus), and she was also being monitored by the endocrinology department for euthyroid goiter. The physical examination showed frontoparietal hair loss in a triangular-shaped pattern (Fig. 1 A) and diffuse thinning on the crown (Fig. 1 B). These findings were consistent with male-pattern female hair loss grade II in the Ebling classification system. The patient also had hirsutism (Ferriman-Gallwey score 9), located predominantly on the face and sides of the neck but also in the chin area (Fig. 2). Examination of the external genitalia revealed an enlarged clitoris. There were no other signs of virilization, such as voice deepening or increased muscle bulk.


Considering the physical findings, we requested blood tests with complete blood count, biochemistry, erythrocyte sedimentation rate, thyroid hormones, and iron profile. The results were all within normal ranges. A hormone study showed hyperandrogenism, with elevated testosterone levels (4.06ng/mL; normal range, 0.20-0.80ng/mL). The tests also showed a level of 28nmol/L for sex hormone binding globulin (normal range, 11-124nmol/L) and a free testosterone index of 45 (normal range, 1.6-6). Free testosterone is the biologically active fraction of testosterone. Androstenedione, dehydroepiandrosterone sulfate, and 17-hydroxyprogesterone levels were all within normal limits. Estradiol levels were high due to peripheral aromatization of testosterone.
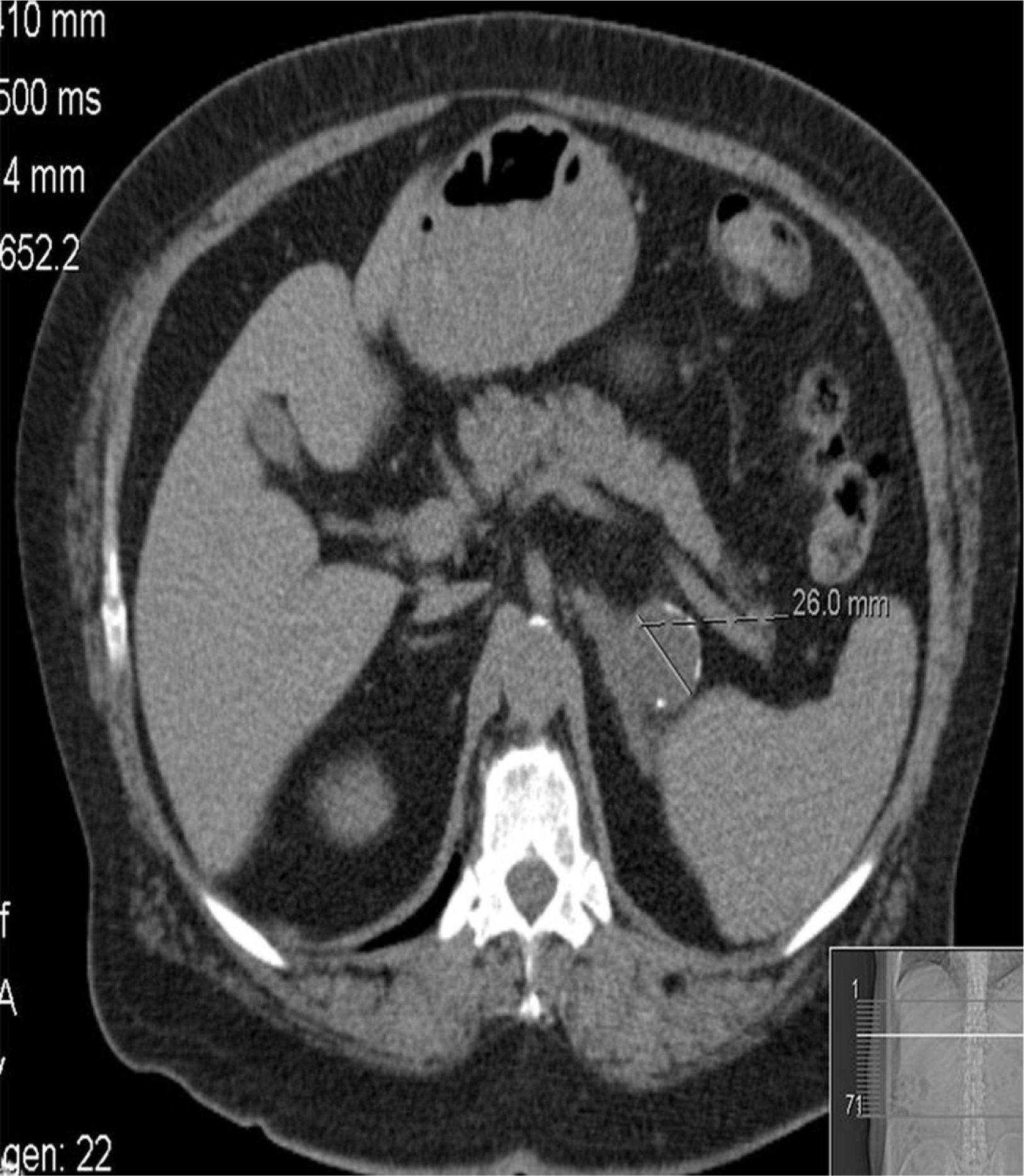
The results suggested an ovarian tumor and we ordered a vaginal ultrasound, which revealed no alterations. The patient was referred to the endocrinology department for further testing, including tumor marker and imaging tests. Prolactin and cortisol tests were normal, as were the results for all tumor markers analyzed except carcinoembryonic antigen, with a level of 14.5ng/mL (normal range, 0-5ng/mL). An abdominal computed tomography scan showed images consistent with a left adrenal tumor (Fig. 3). Magnetic resonance imaging of the pelvis showed no signs of an ovarian tumor. With these findings, it was decided to perform a left adrenalectomy, but the patient continued to show high testosterone levels (4.06ng/mL; normal range, 0.20-0.80) and a high free testosterone index (42.6; normal range, 1.6-6) after the operation. Finally, given the strong suspicion of hyperandrogenism of ovarian origin, we performed a bilateral adnexectomy.
The histologic study confirmed a diagnosis of Leydig cell tumor, hilar type, in the right ovary. At the time of writing, 2 months after the adnexectomy, the patient's testosterone levels have returned to normal and there are evident improvements in her hirsutism and alopecia.
Alopecia and hirsutism can be the presenting manifestation of a tumor,2 as shown by the case reported herein. Hilar Leydig cell tumors of the ovary are very rare and account for just 0.5% of all ovarian tumors. Accordingly, very few cases have been described in the literature. Although benign, these tumors frequently cause virilization, with increased androgen production,3–5 and they are also associated with an increased risk of thromboembolism.6 Leydig tumor cells in the ovary can be very small and may go undetected in imaging studies. This is why adnexectomy is frequently performed as part of a diagnosis of exclusion.7 Adnexectomy of just the affected ovary is an option in premenopausal women. The ovary to be removed is identified during surgery by measuring testosterone levels in the ovarian veins.8
Hyperandrogenism, particularly with signs of virilization, is very uncommon in postmenopausal women and tends to be due to tumors (mainly of ovarian or adrenal origin).9 Other causes that should be ruled out, however, are drugs, pituitary disorders, and the ectopic production of hormones by tumors. The severity of the hyperandrogenism, the patient's age, and the speed with which signs and symptoms appear are all important diagnostic clues.
Please cite this article as: Berbegal L, Albares MP, De-Leon FJ, Negueruela G. Alopecia e hirsutismo en una mujer posmenopáusica como forma de presentación de un tumor de células de Leydig hiliar del ovario. Actas Dermosifiliogr. 2015;106:676–678.


