


Ketoprofen, (RS) 2-(-benzoylphenyl)-propionic acid (C16H14O3), is an arylpropionic acid derivative belonging to the nonsteroidal anti-inflammatory drug family. Synthesized by Rhone-Poulenc SA in the 1960s and marketed internationally since 1973, the drug is used mainly for the treatment of musculoskeletal diseases because of its anti-inflammatory and analgesic properties.1 It is frequently the cause of allergic contact dermatitis and photodermatitis, which was first described in 1985 by Alomar.2 Cross-reactions of unknown origin have also been reported with diphenyl ketone, cinnamic alcohol, and cinnamic aldehyde.1,3–6
We present the case of a patient with photoallergic contact dermatitis to dexketoprofen that appeared 7 years after allergic contact dermatitis to cinnamic aldehyde, hexyl cinnamaldehyde, and 3,4 methylbenzylidene camphor. This is the first report of such an association.
The patient was a 48-year-old woman who was referred to our dermatitis unit with sudden appearance of lesions on the face, trunk, and limbs. The lesions were intensely pruritic after the application of 2 sunscreens (Piz Buin In Sun FPS 50 and ISDIN Fusion gel FPS 50). The patient had used the sunscreen all over her body on 3 consecutive days 30minutes before sun exposure. She also reported that the lesions worsened after using body oil the following day.
Physical examination revealed erythematous edematous plaques with micropapules, mild desquamation, and fissures on the parts of the skin exposed to the sun (Figure 1). After evaluation at the clinic, she was prescribed betamethasone valerate 0.1% ointment twice daily for 2 weeks, after which time her lesions resolved completely.

The patient also reported a 2-year history of very pruritic erythematous lesions on the neck that were occasionally exudative with desquamation and progressed as outbreaks lasting several weeks after application of various colognes and perfumes. Patch testing at our clinic 7 years earlier confirmed a diagnosis of photoallergic dermatitis to dexketoprofen and fenofibrate.
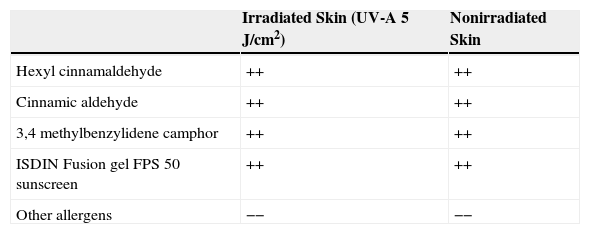
Given her clinical history, photopatch testing was repeated with the standard series of the Spanish Contact Dermatitis and Skin Allergy Research Group (GEIDAC), fragrances (Chemotechnique Diagnostics), and sunscreens (Marti-Tor), as well as her own products, namely, Piz Buin In Sun FPS 50 and ISDIN Fusion gel FPS 50. The tests were performed in duplicate on her back using mostly aluminium chambers (Finn Chamber) and hypoallergenic tape (Scanpor). They were applied under occlusion for 48hours and with exposure to UV-A radiation at 5J/cm2 in 1 of the 2 allergen series. The other series was covered with a black cloth. The results were read at 48 and 96hours and classified according to the guidelines of the Spanish Photobiology Group (Table 1).7,8
The patient, who was sensitized to dexketoprofen, was therefore diagnosed with allergic contact dermatitis to cinnamic aldehyde, hexyl cinnamaldehyde, and sunscreens containing 3,4 methylbenzylidene camphor as a filter. The results of testing with ISDIN Fusion gel FPS 50 had present relevance, since the sunscreen contained the above-mentioned chemical filter.
Ketoprofen is the main photoallergen in Spain. It yields positive results in 2.5% of photopatch tests, with present or past relevance in 95% of these cases.9 Most authors do not differentiate between sensitization to ketoprofen and sensitization to dexketoprofen, since the former is also considered a marker of sensitization to its active isomer, dexketoprofen, and vice versa.9 Several studies support the association between photosensitization to ketoprofen and contact sensitization with cinnamic aldehyde/alcohol, fragrance mix (cinnamic alcohol, cinnamaldehyde, and hydroxycitronellal), fenofibrate, and benzophenone-3.1,3–6,9,10 Some authors feel that these findings could be explained by cross-reactions based on molecular similarities and the high reactivity induced by the presence of a benzene ring attached to a ketone group, which is formed by exposure to sunlight (Figure 2).3,4,6 However, the exact causative mechanisms remain unknown. Consequently, it could be necessary to evaluate sensitization to cinnamic aldehyde and cinnamic alcohol in patients with photoallergic contact dermatitis to ketoprofen/dexketoprofen according to recommendations for a European photopatch test baseline series.10

Reaction induced by UV-A radiation on the dexketoprofen molecule, which is ruptured, leading to the formation of a benzene ring attached to a ketone group. The red circle indicates high reactivity. This group is found in the molecular structures of benzophenone-3, cinnamic alcohol, and fenofibrate and would explain the high frequency of cross-reactions.
In conclusion, sensitization to hexyl cinnamaldehyde and 3,4 methylbenzylidene camphor has not been reported in patients with photoallergy to ketoprofen, dexketoprofen, or both, as in the patient we describe. In our opinion, the nature of the observation in the case of hexyl cinnamaldehyde would be a cross-reaction, which is frequent and well documented with cinnamic aldehyde and cinnamic alcohol (whose molecular structure is similar). In the case of 3,4 methlybenzylidene camphor, the nature of the association would probably be more anecdotal.
Please cite this article as: Rubio-González B, Ortiz-de Frutos F. Eczema alérgico de contacto a aldehído hexil cinámico, aldehído cinámico y 3,4 metilbencilideno alcanfor en un paciente con dermatitis fotoalérgica de contacto previa a dexketoprofeno. Actas Dermosifiliogr. 2015;106:146–148.


