

Fragrances are a large group of substances and the second most common cause of allergic contact dermatitis in Spain.
These potential allergens are extremely common and the general population is subject to continuous exposure on a daily basis.
While the fragrance markers included in the current Spanish standard patch test series are good, there is room for improvement. New markers that have emerged in recent years have proven to be of value in standard series used in other countries. Diagnosing fragrance allergy has taken on even greater importance since the European Union added 26 fragrances to its list of mandatory ingredients to be specified on product labels. The aim of this review is to provide an update on allergic contact dermatitis to fragrances. We examine the main sources of exposure and clinical manifestations of this condition and propose a diagnostic and treatment protocol.
Las fragancias son un grupo amplio de sustancias que representan la segunda causa más frecuente de dermatitis de contacto alérgica en nuestro medio. Son alérgenos ubicuos en nuestra sociedad a los cuales nos exponemos de manera continua y diaria. Actualmente, la batería estándar española tiene buenos marcadores para su detección, pero no ideales. En los últimos años han surgido nuevos marcadores que han sido incluidos en baterías de otros países y han demostrado ser rentables. El diagnóstico de esta entidad adquiere mayor importancia a partir de la entrada en vigor de la ley que obliga a la industria a especificar una lista de 26 ingredientes considerados fragancias en productos comerciales. El objetivo de este artículo es realizar una actualización en la dermatitis de contacto alérgica a fragancias. Revisamos las principales fuentes de exposición, las manifestaciones clínicas y proponemos un protocolo de diagnóstico y manejo terapéutico de estos pacientes.
Fragrances are a large and heterogeneous group of chemical compounds and the second most common cause of contact allergy in our geographical area1 after metals.2–5 Estimated prevalence in the general population is 1.7% to 4.1% according to findings from various studies.6,7
Fragrances are ubiquitous allergens to which we are continuously exposed on a daily basis. Their most obvious use is in commercial perfumes and colognes. In addition, given their odiferous properties and ability to mask odors, they are widely used in cosmetics, household cleaning products, industrial products, topical medications, aromatherapy products, and even in some foods and spices.8 Consequently, avoiding contact with these allergens is a difficult task for patients who are sensitized to fragrances.
In recent years, both official institutions and industry have become aware of the problems brought about by allergy to fragrances, and important changes to legislation have been made. Until a few years ago, manufacturers were not required to disclose chemical compounds in their products if they were defined as fragrance ingredients. Patients allergic to these chemicals had to avoid any household or personal hygiene products containing fragrances, and the widespread use of these ingredients considerably limited their daily activities. Since 2005, European Union regulation has required 26 fragrances that are known contact allergens to be specified on the labels of household and cosmetic products.9–11 This change in the regulation marked a turning point in the management of fragrance-allergic patients and means that patients are no longer limited to using perfume-free products, but are recommended to avoid only those products containing ingredients to which they are allergic.6,9,11 This change also makes it more worthwhile to administer a specific series of fragrance tests in patients who have a positive reaction to the fragrance allergy markers in the standard series.1
The primary objective of this article is to update information on allergic contact dermatitis caused by fragrances. We review the main sources of exposure and the usual clinical manifestations and we propose a protocol for the diagnosis and therapeutic management of such allergies.
Concepts and LegislationBelow, we provide a series of definitions that will help the reader understand the following sections of the review. We also provide an update on current legislation with respect to mandatory labeling of fragrance ingredients.
- 1.
Fragrance: According to the International Fragrance Association (IFRA) a fragrance ingredient is any basic substance used in the manufacture of materials for its odiferous, odor-enhancing or blending properties.5 These substances can be natural extracts or synthetic chemical compounds.12
- 2.
Natural fragrance: Natural fragrance materials are obtained from nature. Most come from plants and are found in flowers, leaves, stems, bark, fruits, or other parts of the plant. Natural fragrances can be extracted using techniques such as distillation, enfleurage (solvent extraction), and maceration. Exceptionally, animal products such as deer musk are used. A natural extract can be composed of a few ingredients or comprise a complex mix of several different ingredients, both major and minor, that account for the complexity of the odor (eg, essential oils and balsams).5,6
- 3.
Synthetic fragrance: Synthetic fragrances are basic, well-defined chemical compounds with a simple odor. They are not obtained directly from nature, but are synthesized artificially in a laboratory. Today, they are the most widely used fragrance materials for reasons of cost, purity, compatibility, and quality control.5
- 4.
Perfume: Perfume is a creative composition or product composed of anything between 10 and 300 fragrance materials, which are generally diluted in ethanol to form an alcohol-based solution. The creation of perfumes, or perfumery, is an ancient art involving the careful selection and quantification of ingredients to create a composition with specific odors that make a product attractive to one's sense of smell.5
- 5.
Masking fragrance: Masking fragrance is used mainly in cosmetic products and topical medications labeled as inodorous in order to mask unpleasant odors from the chemicals that are the active ingredients in the product.13
- 6.
Balsam: Balsam is a liquid and almost transparent aromatic substance obtained by making incisions in the bark of certain trees. However, once the liquid comes into contact with the air, it becomes viscous and colored and its essential oils are transformed into resin and benzoic and cinnamic acid.14
- 7.
Essential oils: Essential oils are aromatic substances extracted from various plants or from a small number of animals. They can also be synthesized from coal or petroleum. Essential oils are composed of terpenoids and phenylpropanoids, which are volatile compounds. Essential oils are extracted by distillation, enfleurage, solvent extraction, expression, and supercritical fluid extraction. Aromatherapy is based on essential oils that are applied topically or inhaled to promote physical and psychological well-being. They are widely used and have become increasingly popular in recent years.5,6
- 8.
Legislation and safety: Two main organizations are responsible for regulating the use of fragrances in industry. The Research Institute of Fragrance Materials (RIFM) was founded in 1966 in the United States to generate, evaluate, and disseminate scientific data on the use of fragrances in consumer products.15 The IFRA was created in 1973 and is responsible for using these data to monitor safety in the use of fragrances and for creating industry codes of practice and guidelines. This organization makes recommendations on limiting or prohibiting the use of specific substances and on testing new fragrances to rule out toxicity before they come onto the market.5,12 Despite the work carried out by these institutions, the ingredients used in industry have been kept secret for many years. In 2003, in accordance with the seventh amendment to the European Directive on Cosmetic Products,10 the European Union created a list of 26 ingredients that must be listed on cosmetic product labels (Table 1) if the content exceeds ≥10ppm for leave-on products and ≥100 for rinse-off products; this list includes all the substances present in the fragrance mixes I and II used in patch tests. Some months later, the same measure was applied to household products, such as detergents and similar products. This directive was implemented in Spain in 2005 after the publication of Royal Decree 209/2005 (Official State Journal, February 26, 2005). Compliance with legislation on cosmetic products is generally good in Spain; however, the same cannot be said about household products. The directive, while adequate, could be improved, since several studies in Europe have revealed the need to review and modify the list of 26 allergens9 as a result of the discovery of new fragrances that cause contact eczema.
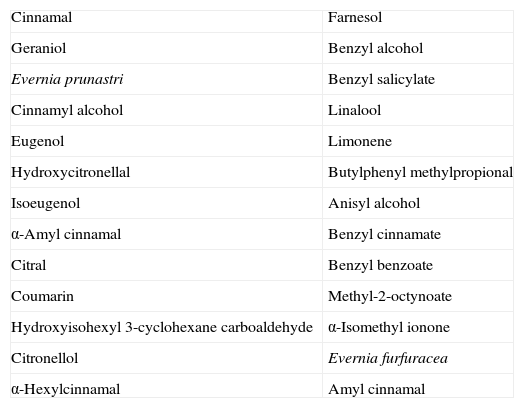
Table 1.List of the 26 Fragrances that must be Specified on the Labels of Cosmetic Products (When Present at a Concentration of ≥10ppm in Leave-on Products and ≥100ppm in Rinse-off Products), According to the Seventh Amendment to the European Directive on Cosmetic Products.
Cinnamal Farnesol Geraniol Benzyl alcohol Evernia prunastri Benzyl salicylate Cinnamyl alcohol Linalool Eugenol Limonene Hydroxycitronellal Butylphenyl methylpropional Isoeugenol Anisyl alcohol α-Amyl cinnamal Benzyl cinnamate Citral Benzyl benzoate Coumarin Methyl-2-octynoate Hydroxyisohexyl 3-cyclohexane carboaldehyde α-Isomethyl ionone Citronellol Evernia furfuracea α-Hexylcinnamal Amyl cinnamal
Today, most people are exposed to fragrances daily through many and varied sources.6 Exposure may be as a consumer or in an occupational setting.
ConsumerThe source of fragrances we are most commonly exposed to as consumers are cosmetic products, which include commercial perfumes, cologne, and personal hygiene products of all kinds. However, fragrances are found everywhere: in household products, medications, and even food products.
Cosmetic ProductsFragrances16,17 are the most frequent cause of allergy to cosmetic products, even more so than preservatives. Commercial perfumes and colognes have the highest concentration of fragrances, containing 20%-30% and 4%, respectively5,18; moreover, a single perfume can contain between 10 and 300 different fragrances.19 A study analyzing the composition of 10 prestigious perfumes revealed that they contained a mean of 5 allergens from those present in fragrance mix I; more recently marketed perfumes only contained a mean of 2.8 allergens.20 The difference could be the result of growing industry awareness of allergy to fragrances. The most common allergens in perfume were hydroxycitronellal and geraniol; the least common was α-amyl cinnamal.20
Fragrances can also be found in products such as shampoos, conditioners, soaps, deodorants, wet wipes, body oils, moisturizing creams, and make-up. Yazar et al.19 analyzed 206 commercial cosmetic products (shampoos, conditioners, gel, and wipes), excluding perfumes and colognes, and found fragrances in 90% of them. The most common were linalool (38%), hexylcinnamal (32%), butylphenyl methylpropional (29%), limonene (28%), and citronellol (20%). Children's cosmetic products contain fewer and less concentrated allergenic fragrance ingredients than those of adults.21
Heisterberg et al.22 recently found that the sources most commonly associated with allergy to fragrances are deodorants, even more so than colognes and perfumes. The reason may be that the area of application is occluded and contains hair follicles that enable the allergens to enter the body easily.22,23 One series of 1016 patients revealed a significant correlation between axillary eczema and allergy to fragrances.24 In a study of 73 deodorants sold in 5 European countries, eugenol and geraniol were found to be the most common fragrance ingredients.25 Furthermore, all the fragrance components found were at a much higher concentration than in other personal hygiene products. Another important allergen in allergic contact dermatitis caused by deodorants is the fragrance hydroxyisohexyl 3-cyclohexane carboxaldehyde, commonly known as lyral26 (Fig. 1).

Contact dermatitis due to fragrances manifesting as axillary eczema associated with the use of a deodorant containing lyral. A, Erythematous lesions with an eczematous appearance that had appeared on the right axilla several weeks previously. B, Patch test with lyral showing a positive reading at 72hours.
Fragrances are also found in oral hygiene products, such as toothpastes and mouthwashes: several cases of allergy to eugenol in these products have been reported.13
Special mention must be made of cosmetic products classed and marketed as fragrance-free, since even these can contain perfumes that mask the unpleasant odors of other ingredient .13
Household ProductsMost household products, such as detergents, fabric softeners, air fresheners, cleaners, and polishes, also contain fragrances. Allergy to the fragrances in these products usually manifests as hand eczema.27 Limonene is the most common fragrance in several series,19,27 while eugenol and hydroxycitronellal are much less common than in cosmetic products.
Topical MedicationsSeveral topical medications have been reported to cause allergic contact dermatitis because of their fragrance content. These include creams and salves containing corticosteroids, antibiotics, antiseptics, healing agents, other medications used to treat wounds, anti-inflammatory agents, antimycotic drugs, and antipruritic agents. Application to damaged and vulnerable skin (eg, wounds, ulcers, and eczema) is an important route of sensitization and predisposes patients to multiple sensitizations.28 This situation is particularly common in patients with leg ulcers whose wounds are treated on a daily basis with a variety of topical agents. Balsam of Peru was found in 40% of patients receiving this care who were studied because they had eczema.29 Fragrances were involved in 3.8% of 3378 cases of medication-induced contact dermatitis, which mainly affected women and the legs.28 The capacity for developing allergy to fragrances seems to be more common than that for developing allergy to other allergens, such as antibiotics, excipients, rubber accelerators, and corticosteroids.30 Furthermore, fragrances are not an essential component of topical agents, and several authors have stressed the need for improvements in legislation governing products of this type.31,32
Clothing/FabricClothing and fabrics can contain fragrances after washing with softeners, especially industrial softeners.
FoodsFragrances are occasionally used to give taste to certain foods, such as cough syrup, chewing gum, soft drinks, and ice cream. Some fragrances are synthetic, whereas others, such as clove, vanilla, or cinnamon, are natural. Ingestion of these allergens can lead to systemic contact dermatitis, which manifests as hand dermatitis, nonspecific dermatitis, and reactivation of eczema in areas previously exposed to topical medication.33
OccupationalOccupational contact allergy due to fragrances has received little attention in the literature.6 It is interesting to note that while outside the occupational setting these substances represent the second most common cause of contact allergy in the workplace, they are not even among the 10 most frequent allergens.34 In the literature on occupational allergies, fragrances tend to be relegated to a secondary role, because they are rarely the only etiologic factor involved; in fact, in most cases, dermatitis is mainly irritant.5 Furthermore, when a worker presents with allergy to fragrances, the condition is usually attributed to their contact with fragrances as a consumer.35
Workers can come into direct contact with fragrances in several jobs. Below, we present such contact according to whether the setting is the industrial sector or the services sector.
Industrial SectorAllergy to fragrances is to be expected in workers in the perfumery and cosmetics industry. In 1948, Bonnevie36 reported a series of cases in which all the workers in a perfume factory became sensitized to cinnamic aldehyde. More recently, Schubert37 found 6 cases of allergic contact dermatitis induced by fragrances among perfume industry bottlers who were sensitized to geraniol, benzaldehyde, and cinnamic aldehyde. Cases have also been reported among chemists and laboratory technicians in this sector.38,39
Metalworking and other industrial processes use cutting oils (coolant and lubricant) comprising several substances, including fragrances. A study from the Informationverbund Dermatologischer Kliniken (IVDK) of 160 workers in the metalworking industry found that fragrances were the third cause of sensitization to these oils.40 Cases can also be found in the paint, rubber, insecticide, paper, and food industries.
Service SectorThe service industry workers with the highest frequency of allergy to fragrances are hairdressers, beauticians, and aromatherapists, whose profession involves contact with these substances. Occupational contact dermatitis is a significant health problem among hairdressers. In 2009, a Polish center studied 121 hairdressers with hand dermatitis: 70% were sensitized to 1 or more of the allergens from the standard series, and of these, 4.5% were allergic to fragrances, which were the 12th most common cause of allergy after hair dye, metal, and preservatives.41
Aromatherapy has become increasingly popular in recent years. Several cases of allergic dermatitis induced by essential oils have been reported, especially among masseurs and beauticians. Most cases involve women with hand dermatitis who were sensitized to several allergens.42,43
Workers in the health care sector are also affected by exposure to these allergens, especially in odontology (eugenol),44,45 as are workers such as cooks and waiters who come into contact with foods or spices.
EpidemiologyToday, approximately 3000 substances are used as fragrances.1 Although fragrances are widespread allergens with which almost all of the general population comes into contact,5 the percentage of individuals who are allergic to fragrances is relatively low. In contrast, in absolute numbers, contact allergy to fragrances is common and constitutes the second most frequent cause of allergic contact dermatitis in our environment.5 At least half of all fragrance-allergic individuals do not associate their symptoms with contact sensitization to these substances.9 The exact frequency of allergy to fragrances in the general population is difficult to determine.13 A review published in 2009 analyzed 19 studies that performed patch testing with fragrance markers in the general population and obtained a mean prevalence in adults of 3.7% for fragrance mix I and 1.1% for balsam of Peru (Myroxylon pereirae).46 No studies of this type have been performed for fragrance mix II. The frequency of allergy to fragrances is lower in children and increases with age, probably because of repeated exposure throughout life.46,47
Determining the prevalence of sensitization in patients with eczema who consult a dermatologist is somewhat easier, as confirmed in numerous articles on the subject. However, these data are thought to be underestimated, since patients often identify the problematic products and simply stop using them without consulting their physician.1,5 The Spanish Surveillance System on Contact Allergies (REVAC) collected data from 5 Spanish hospitals on 1161 patients48 who had undergone patch testing in 2008 and found that 9.08% were sensitized to fragrances (fragrance mix I, 4.64%; balsam of Peru, 4.44%). A retrospective 4-year study on fragrance contact allergy in a Spanish hospital analyzed data from 1253 patients who had undergone patch testing with a series containing 4 fragrance markers (fragrance mix I and II, balsam of Peru, and lyral). In that study, 9.3% of the population had a positive reading to at least 1 of these markers.1
The percentages reported by the IVDK, which studied 40 790 patients from several European centers between 2005 and 2008, were somewhat higher: 15.1% of patients were sensitized to fragrances. According to the findings of the North American Contact Dermatitis Group, this prevalence increased to 23.4% in the United States, with positive results to fragrance mix I in 11.5% of cases and to balsam of Peru in 11.9%.49 Some authors believe that these geographical variations could be partly due to the allergens used in testing, the differences in concentrations used, and country-specific preferences for different fragrances.13
When gender is analyzed, most studies show greater sensitization among women, probably because of their greater contact with cosmetic and household products; however, other studies found no differences according to gender,5,50 and a greater prevalence has even been reported among men.1
The fragrances that most commonly cause dermatitis in the patients studied vary significantly by region. In European studies, the most commonly detected fragrances were Evernia prunastri, isoeugenol, and cinnamal; geraniol was one of the least prevalent. However, a Spanish series found geraniol to be the most prevalent fragrance in the patients tested, followed by eugenol and cinnamic alcohol; therefore, we do not feel geraniol should be withdrawn from the standard battery in Spain.1
Conflict of InterestsThe authors declare that they have no conflicts of interest.
Please cite this article as: Arribas MP, et al. Dermatitis de contacto alérgica por fragancias. Parte I. Actas Dermosifiliogr. 2012;103:874–9.


