

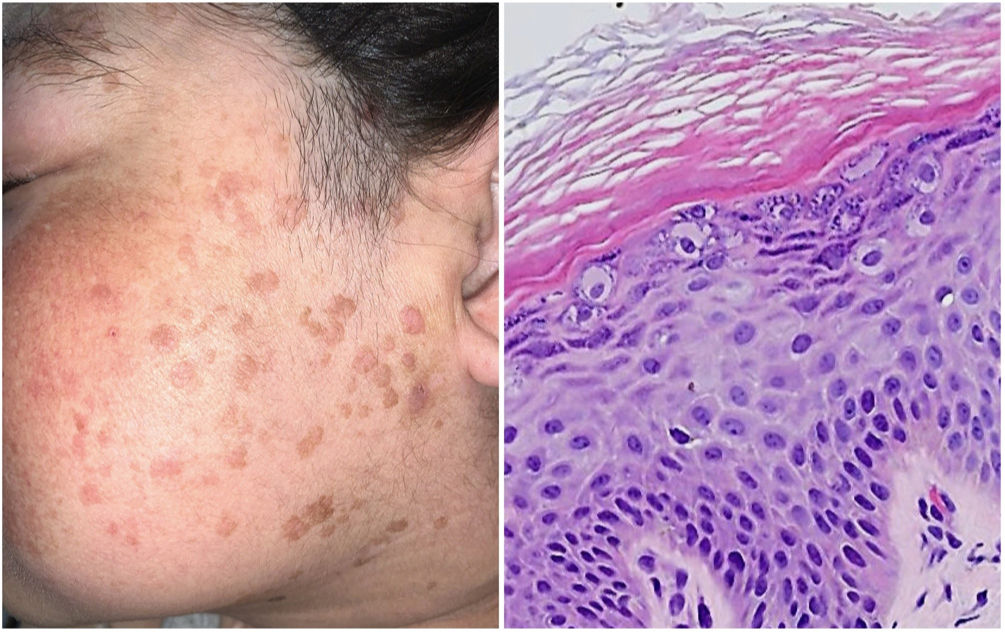
A 39-year-old woman came to the clinic with asymptomatic flesh-colored verruciform flat papules on her face that had first appeared 5 years earlier. The patient had undergone a kidney transplant owing to lupus glomerulonephritis, with chronic active rejection. She was receiving 3 sessions of hemodialysis per week, as well as meprednisone 4mg/d and tacrolimus 7mg/d.
Histopathology revealed enlarged keratinocytes with a pale blue cytoplasm in the upper layers of the epidermis. These findings were compatible with epidermodysplasia verruciformis (Fig. 1).
Epidermodysplasia verruciformis is an uncommon disease. It is characterized by susceptibility to human papillomavirus infection that predisposes to multiple skin tumors on areas exposed to sunlight. The disease may be genetic in origin (mutations in EVER1/TMC6, EVER2/TMC8, RHOH, MST1, CORO1A, and ECM1) or acquired (iatrogenic or associated with HIV infection). The most common skin manifestations are flat hypo- and hyperpigmented macules, verruca-like papillomatous lesions, seborrheic keratosis, or reddish pityriasis versicolor. The lesions may progress to various types of neoplasm, the most frequent of which is squamous cell carcinoma.
In patients with iatrogenic acquired epidermodysplasia verruciformis, immunosuppressive therapy should be modified if possible.


