


A 64-year-old woman with severe actinic damage presented with a pigmented lesion of recent onset on the external aspect of her left leg. The clinical examination showed an irregular pigmented macule with a lentiginous appearance and measuring 7 mm at its widest point; the surrounding skin showed signs of severe sun damage, with multiple solar lentigines (Fig. 1).
Comment
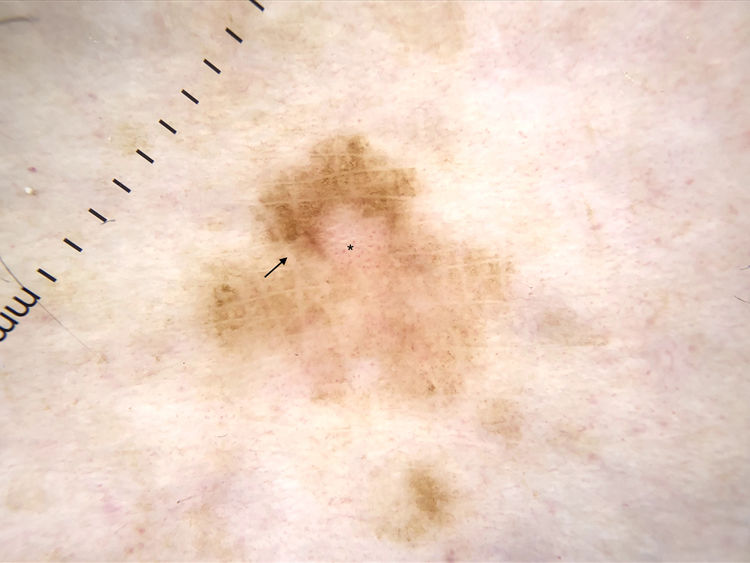
Polarized light dermoscopy showed a discrete irregular pigment network, light-brown structureless areas, hypopigmented areas, and sparse, irregularly distributed, dots. One particularly remarkable finding was the presence of prominent skin markings in the form of intersecting lines that were paler in color than the rest of the lesion and interrupted other structures. Also visible were dotted vessels in the hypopigmented areas that were more visible than those in the surrounding skin (Fig. 2).
 and the dotted vessels in the hypopigmented areas (asterisk).")
Dermoscopic image showing an irregular pigment network, light brown structureless areas, hypopigmented areas, and sparse irregularly distributed dots. Note the prominent intersecting skin markings paler in color than the rest of the lesion (arrow) and the dotted vessels in the hypopigmented areas (asterisk).
Considering the clinical context (a flat pigmented lesion of recent onset in a patient with severely sun-damaged skin) and the dermoscopic findings, the lesion was excised. The histopathologic diagnosis was melanoma in situ with a lentiginous growth pattern.
The dermoscopic finding of prominent skin markings was recently described as a powerful diagnostic indicator of melanoma in situ versus atypical nevus, particularly in sun-damaged areas of the skin.1 These markings, which are associated with high levels of interobserver agreement, are intersecting linear furrows, lighter in color than the rest of the lesion. They have been linked in particular to melanoma in situ or melanoma with a low Breslow thickness located on the lower limbs.2
Lallas et al.1 reported that, while less common, prominent skin markings can also be found in other lesions, such as, in order of frequency, Reed nevus, melanocytic nevus, seborrheic keratosis/solar lentigines, Bowen disease, and basal cell carcinoma.
Although the significance of prominent skin markings has generated some controversy,3 this dermoscopic feature has proven to be a powerful predictor of melanoma after adjustment for sun damage and age in the studies in which it has been described.4 Other more common dermoscopic features associated with melanoma in nonfacial chronically sun-damaged skin are angulated lines, granularity, and groups of atypical dots.5
The atypical vascular pattern is more common in invasive melanoma than in melanoma in situ.5 Uniform, regularly distributed, dotted vessels, however, are characteristic of flat lesions, like the one presented in this case.6
In conclusion, prominent skin markings are a new dermoscopic marker that should raise suspicion in melanocytic lesions and could help increase the early detection of melanoma, particularly in sun-damaged skin.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Álvarez-Salafranca M, Sánchez-Bernal J, Ara Martín M. Líneas cutáneas prominentes: un nuevo criterio de sospecha en lesiones melanocíticas. Actas Dermosifiliogr. 2021;112:451–452.



