





Polyarteritis nodosa (PAN) is a vasculitis that affects small and medium-sized vessel. It is traditionally divided into 2 forms. The cutaneous form is the variant in which the clinical manifestations are limited to the skin, though muscle pain and generalized joint pain may also be reported, and neuritis in areas close to the affected skin. Fever is detected in up to a third of cases. The systemic form affects internal organs, most commonly the kidney, liver, and central nervous system.1
A 50-year-old man was seen in our department for a 5-year history of outbreaks of nodular lesions, initially only affecting the legs, associated with widespread joint pain. In the last year, lesions had also appeared on his arms, and he had developed episodes of fever, weight loss, asthenia, and anorexia. He had been on follow-up at another hospital, where several biopsies had been performed with nonspecific results (a dermal neutrophilic infiltrate, stasis dermatitis, and, in the most recent biopsy, a predominantly lobular panniculitis). He had received no definitive diagnosis. Despite treatment with various drugs, control of his disease had not been achieved; throughout this whole period he had been administered oral corticosteroids, with intermittent courses of colchicine, azathioprine, methotrexate, and ciclosporin. Important blood test results included elevation of the acute phase reactants (AFRs), with elevation of C-reactive protein and erythrocyte sedimentation rate (which had risen to 120mm/h in recent months). Other additional tests, including autoimmunity studies (antinuclear antibodies, extractable nuclear antigen, and antineutrophil cytoplasmic antibodies) and serology (HIV and hepatotropic viruses), were normal or negative.
When the patient first came to our hospital, he presented erythematous plaques with peripheral desquamation, mainly on his lower limbs but also on his upper limbs. Nodules were present beneath the plaques. He also presented edema of the dorsum of the left foot and ankle (Fig. 1,A-C). A biopsy was taken, which was consistent with septal panniculitis (Fig. 1D).
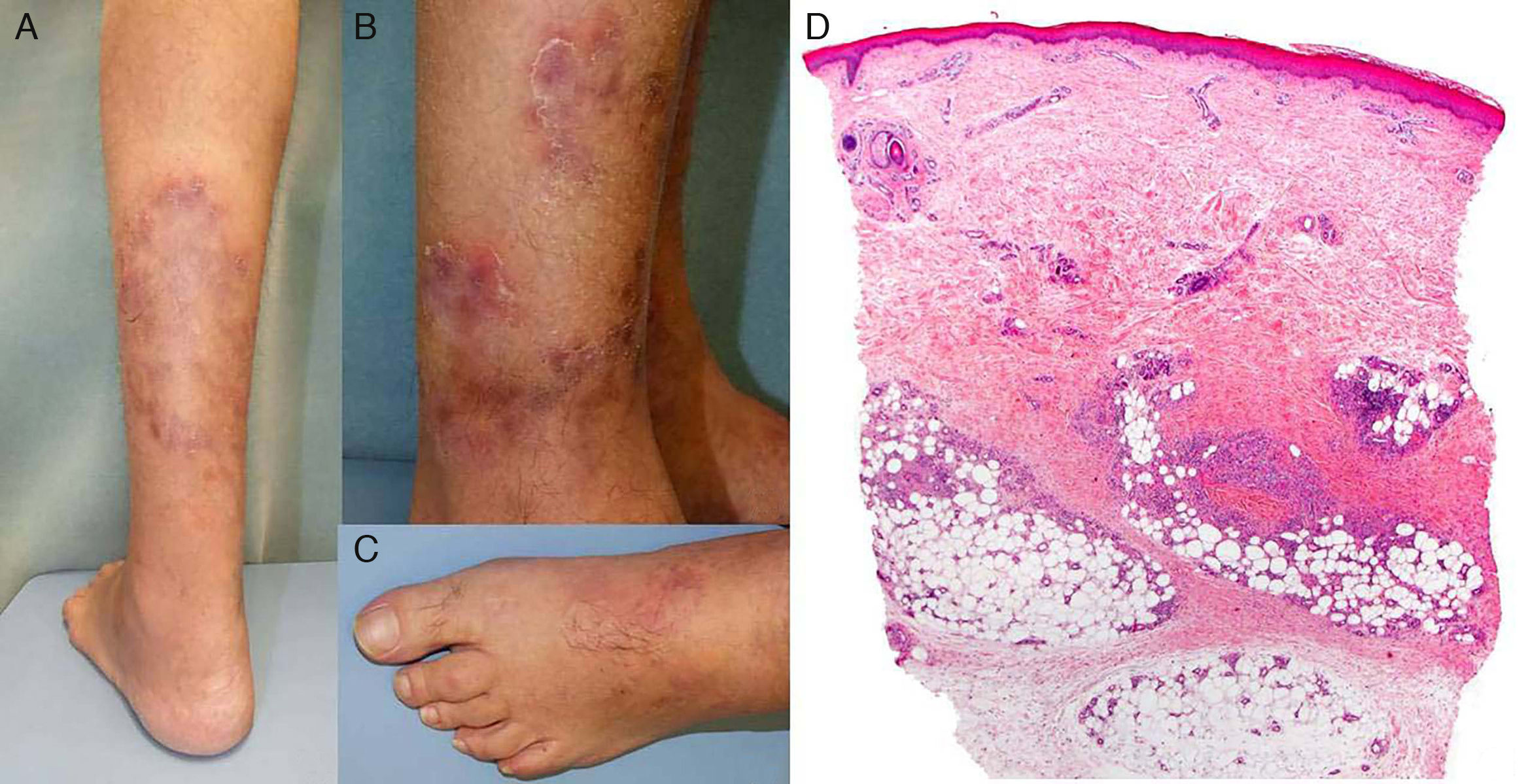
A, Nodules beneath erythematous plaques with peripheral desquamation. B, In greater detail, showing the residual hyperpigmentation. C, Edema on the dorsum of the left foot. D, Skin biopsy showing a normal epidermis and dermis, with lesions in the subcutaneous cellular tissue. Inflammatory infiltrate in the septa. Hematoxylin and eosin, original magnification×4.
Coinciding with tapering of the dose of prednisone, the patient presented a further outbreak at the same sites as the previous outbreak, with purpuric plaques that spread centrifugally, pain, bilateral ankle edema, and fever.
A further biopsy revealed a neutrophilic infiltrate in the small and medium-sized vessels, with fibrinoid necrosis, and a moderate eosinophilic infiltrate (Fig. 2, A andB). Based on these findings, we made a diagnosis of PAN. Given the absence of organ involvement, despite the marked elevation of the AFRs and alteration of the patient's general state of health, we considered this to be cutaneous PAN with an associated systemic inflammatory response.
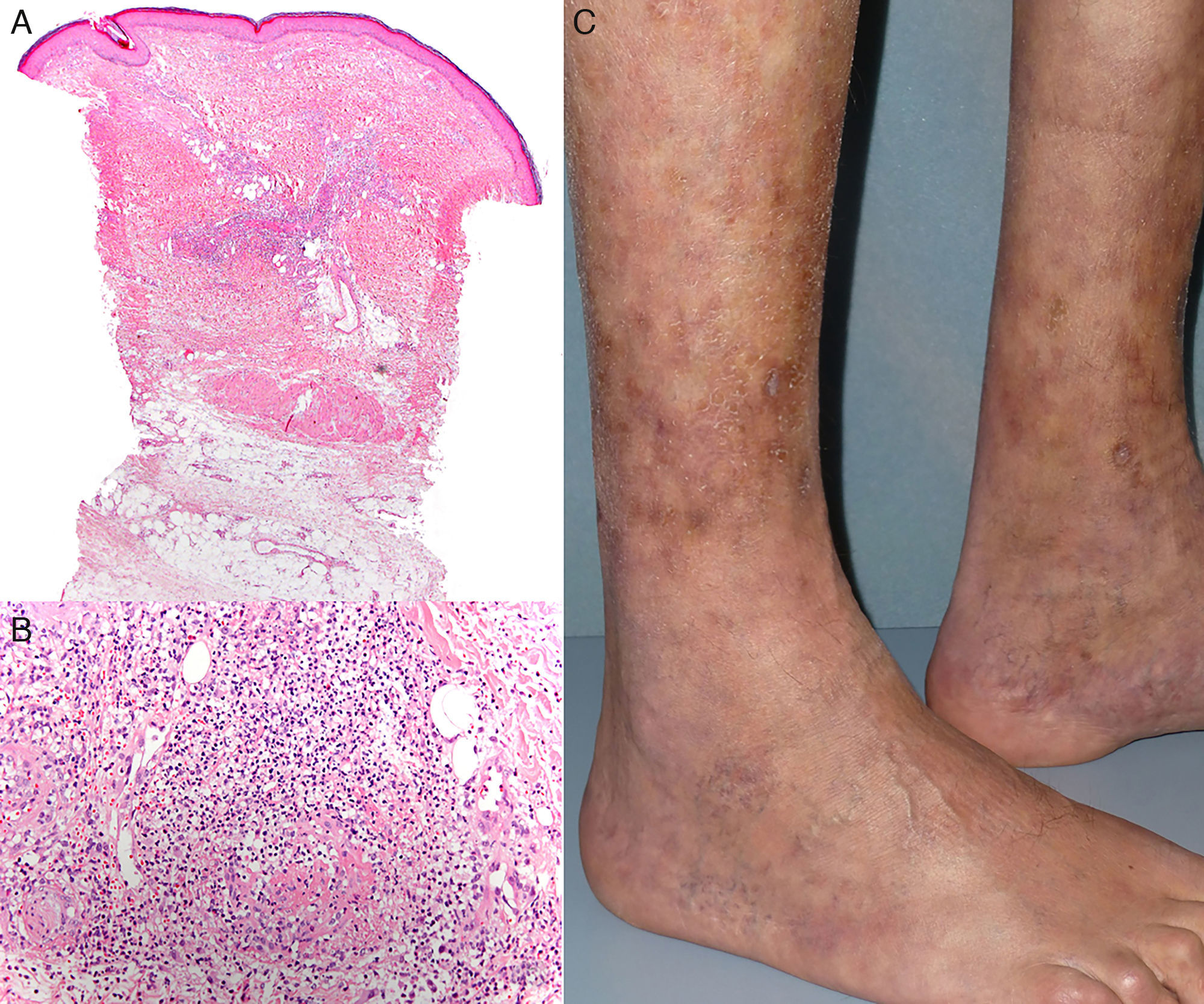
A, Normal epidermis with lesions in the dermis and subcutaneous cellular tissue. Hematoxylin and eosin, original magnification ×4. B, Fibrinoid necrosis and a neutrophilic infiltrate in the medium-sized vessels, with an associated eosinophilic infiltrate. Hematoxylin and eosin, original magnification×20.C, Residual livedo on the legs after starting treatment with infliximab.
After increasing the dose of prednisone to 1mg/kg/d and controlling the acute outbreak, treatment was started with cyclophosphamide and immunoglobulins. However, this did not enable us to reduce the dose of corticosteroids without renewed deterioration. Treatment was therefore commenced with infliximab at a dose of 5mg/kg, which led to a very good response after the first infusion, with complete normalization of laboratory parameters. The dose of corticosteroids was progressively reduced until their withdrawal, with no further outbreaks of lesions in a year of follow-up, except for a residual livedo (Fig. 2C); during this period the patient continued treatment with infliximab every 8 weeks.
The typical clinical manifestations of cutaneous PAN are characterized by outbreaks of painful nodular lesions that leave a residual livedo.1 In the first patient series, dating from 1974, the presence of a starburst pattern was described as a characteristic manifestation of this livedo, and was very similar to that observed in our patient, though we have found no similar descriptions in the recent literature.2
Typically, histology reveals a focal panniculitis around affected arteries. However, if the inflammatory infiltrate is very intense, the panniculitis can be so pronounced that it masks the vasculitis.1
Three subgroups of cutaneous PAN have been described based on the presentation, laboratory tests, and clinical course: class i, in which the cutaneous manifestations are associated with slightly elevated AFRs; class ii, in which constitutional symptoms are also present, with fever and marked elevation of the AFRs; and class iii, in which the cutaneous form progresses to systemic forms of the disease.3 We classified our patient in the second subgroup.
In cutaneous PAN, patients with marked elevation of AFRs are more likely to present inflammatory plaques and edema of the lower limbs. Considering this association as a more severe form of the disease, it has been proposed that the initial management approach should be more aggressive to avoid progression to systemic forms.4
Although the use of TNF inhibitors is not uncommon in the systemic forms of PAN, we have found very few reports in the literature in which this treatment has been required to control cutaneous forms (Table 1).
Treatment With TNF Inhibitors in Cutaneous Polyarteritis Nodosa.
| Patient | Authors, Year, and Reference | Age, y | Sex | Previous Treatments | Duration of Previous Treatments, mo | TNF Inhibitor, Dose | Concomitant Immunosuppressant Treatment | Follow-up, mo | Outcome/Adverse Events |
|---|---|---|---|---|---|---|---|---|---|
| 1 | García-Porrua and Gonzalez-Gay,5 2003 | 47 | Male | Indomethacin, SSZ, MTX | 0 | IFX, 5mg/kg | MTX 15mg/wk | 18 | Resolution/none |
| 2 | Vega Gutiérrez et al.,6 2007 | 14 | Female | OC | NA | IFX, 5mg/kg | No | NA | Resolution/none |
| 3 | Bansal and Houghton,7 2010 | 7 | Female | OC, CY, MTX, IVIG | 14 | IFX, 5mg/kg first dose, followed by 10mg/kg every 4 wk | OC, MTX | 8 | No response (corticosteroid dependence). Response to RTX and CY |
| 4 | Zoshima et al.,8 2013 | 66 | Female | OC, MTX, CsA, TAC, CY, AZA, colchicine, PE, DFPP Lamivudine, adefovir | 156 | ETN, 25mg/wk | OC | 8 | Resolution/none |
| 5 | Campanilho-Marques et al.,9 2014 | 13 | Male | OC, MTX, CY, RTX | 13 | IFX, 5mg/kg | No | 12 | Resolution/none |
| 6 | Valor et al.,10 2014 | 7 | Male | OC, CY | 3.5 | ETN, 25mg/wk | No | 84 | Resolution/none |
Abbreviations: AZA, azathioprine; CsA, ciclosporin; CY, cyclophosphamide; DFPP, double filtration plasmapheresis; ETN, etanercept; IFX, infliximab; IVIG, intravenous immunoglobulin; MTX, methotrexate; NA, not available; OC, oral corticosteroid therapy; PE, plasma exchange; RTX, rituximab; SSZ, sulfasalazine; TAC, tacrolimus.
In conclusion, we have presented a case of cutaneous PAN associated with a systemic inflammatory response and refractory to conventional treatments. It is essential to suspect this disease in patients with nodules beneath plaques showing centrifugal spread, even if histology does not initially support the diagnosis, particularly if there is an associated intense inflammatory reaction that could hide the vasculitis. Patients with cutaneous PAN with very high AFRs will often require management similar to the systemic forms, and TNF inhibitors are an option.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Tous-Romero F, Rodríguez-Almaraz E, Rodríguez-Peralto JL, Postigo-Llorente C. Panarteritis nudosa con patrón de respuesta inflamatoria sistémica: respuesta a anti-TNF. Actas Dermosifiliogr. 2017;108:787–790.


