





The pinna is a complex structure with contour lines that should be conserved during reconstruction.1 One of these lines is formed by the helix, which gives the distinctive shape to the ear. This is also the site of half the malignant tumors that arise in the pinna.2 Techniques for reconstruction are varied and include direct closure, grafts, and skin or chondrocutaneous advancement flaps, where the choice of which to use is guided by the particular needs of each case.3 However, large upper-pole defects remain a challenge for reconstructive surgery.
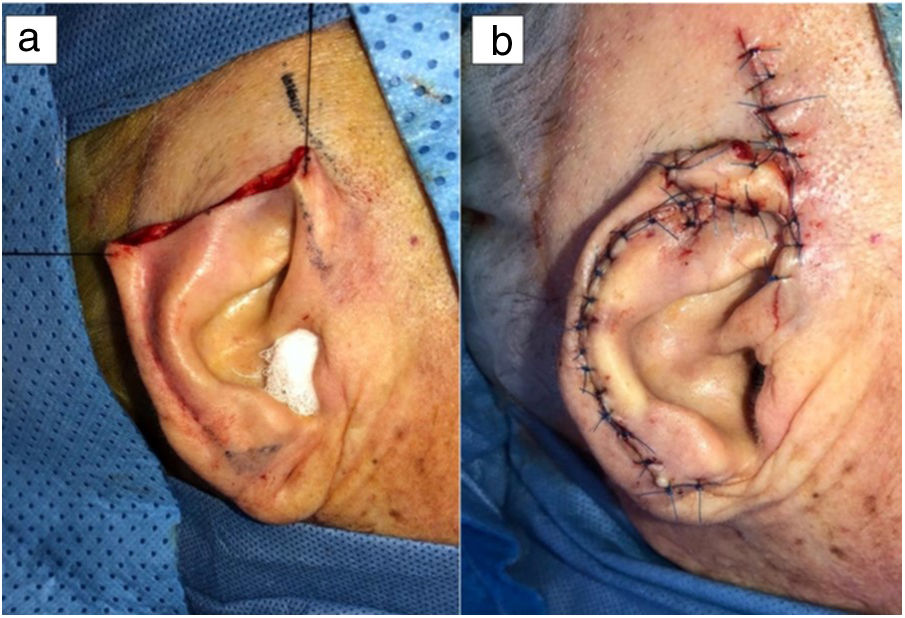
An 85-year-old woman from a remote region of Colombia (Orinoco region), presented with invasive basal cell carcinoma measuring 15 × 15 mm on the upper part of the right helix. The tumor was treated by transfixing resection with lateral margins of 8 mm. The postsurgical defect measured 35 mm in diameter and covered more than one-third of the length of the helix. Use of several flaps in different procedures was ruled out given the patient’s difficulty to travel to our hospital. Instead, the Antia-Buch technique was chosen using 2 flaps, an upper one and a lower one. To construct the flaps, an incision was made in the skin anterior to the ear and the cartilage without cutting posterior skin. Dissection was performed superficially to the posterior perichondrium, such that the flaps only had cartilage in their distal portion. A wedge was cut in the antihelix to enable the flaps to be drawn together. The flaps were advanced and sutured in layers with Vicryl® and Prolene® 5/0 stitches. A V-Y closure was performed on the upper secondary defect (Fig. 1). The outcome 1 week later was a functional pinna with no cup ear deformity (Fig. 2). The patient had an area of superficial necrosis of less than 1 cm that fully re-epithelialized.

Reconstruction of the pinna should seek to preserve its auxiliary function in the auditive process and as a support for glasses.2 The main esthetic objectives of reconstruction include retaining symmetry, preserving a smooth helix with its characteristic form, and preserving skin color and texture.4
There are different reconstructive techniques available and the choice of which to use depends on the site and size of the defects. In the upper helix, defects with no cartilage involvement can be resolved with skin grafts or local skin flaps. Defects of the helix with loss of cartilage may impact the shape of the pinna and so re-epithelization by second intent, grafts, and local skin flaps are insufficient.4 Helical defects of less than 10 mm can be resolved by primary closure or compound grafts.3 Larger defects need chondrocutaneous advancement flaps, such as the Antia-Buch flap, and, if the defects are greater than 20 mm, retroauricular island flaps or temporoparietal fascial flaps with cartilage graft can be used.3
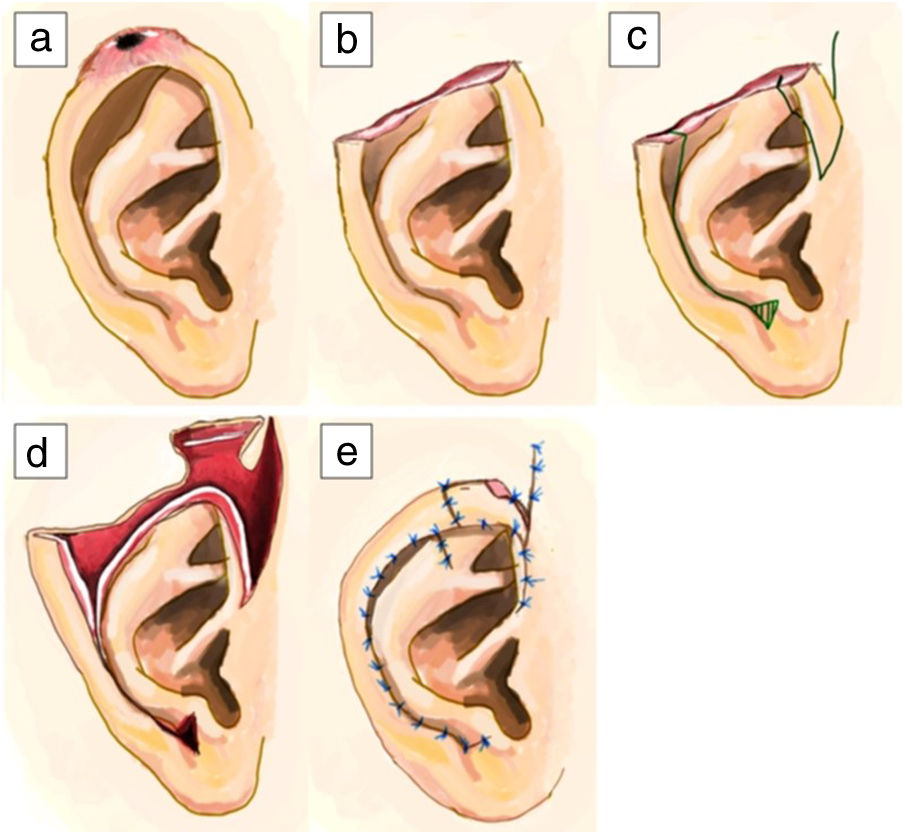
Chondrocutaneous advancement flap of the helix is a simple technique described in 1967 by Antia and Buch to reconstruct the transfixing defects of the helix in a single surgical procedure.5 Depending on the size and site of the defect, 1 or 2 simultaneous flaps may be required. The incisions should be made parallel to the helix in the anterior face of the pinna, including the cartilage, but without making an incision in the posterior skin as the flaps are based on branches of the posterior auricular artery.6 The posterior face of the ear is then dissected to separate the skin from the cartilage.2 This maneuver frees the flaps and allows them to be advanced. Before suturing the flaps, it is necessary to assess whether they are long enough to surround the pinna. If not, cartilage should be cut away from the concha or the antihelix. The secondary defect of the upper flap can be closed with the V-Y technique,7 whereas the inferior flap may require a Burrow triangle to compensate for any redundant tissue (Fig. 3).2
The Antia-Buch technique plays an important role in reconstruction of the upper pole of the ear; however, more complex techniques are preferred for defects measuring more than 20 mm.3 One of the concerns with the Antia-Buch flap for large defects is cup ear deformity. However, modifications to this technique, such as half-moon or wedge cuts of the antihelix and concha can avoid this problem.2,7,8 A main advantage of this technique is that it only requires one operation. This is desirable in patients of advanced age, those with comorbidities,7 or those with difficulties traveling to hospital; 3 conditions often seen in our everyday practice. With this case, we would like to highlight the simplicity and usefulness of this technique for reconstruction of large defects of the pinna in the upper pole, particularly when only one operation is desirable.
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Barrera Gamboa JC, Acosta Madiedo de Hart AE. Colgajo de Antia-Buch para un defecto amplio del polo superior de la oreja. Actas Dermosifiliogr. 2021;112:558–559.


