





Granuloma faciale (GF) is a rare benign inflammatory dermatosis of unknown aetiology, characterized by single or multiple red-brown or violaceous cutaneous nodules or plaques, most frequently occurring on the face. GF is considered a form of localized chronic fibrosing vasculitis.1 Diagnosis is commonly confirmed by skin biopsy, although the histopathological diagnosis of GF may be challenging, because precise histopathological criteria have not been defined. Differential diagnosis is broad and includes inflammatory diseases, malignancies and infections. High resolution ultrasound (HRU) is being used increasingly in dermatology, both for the diagnosis and monitoring of diverse inflammatory dermatoses and tumoral lesions.2 We have not found publications about ultrasonographic features of GF. We aimed to describe the ultrasonographic characteristics of GF in a series of patients.
Patients with biopsy-proven GF who consulted at a Spanish tertiary referral hospital between January 2016 and May 2018 were included. Lesions were assessed using an Esaote MyLab Class C ultrasound machine with 18 and 22 MHz probes. All the sonographic examinations were performed by following published guidelines for studying dermatologic lesions that include grayscale and color Doppler imaging.3 All patients gave oral and written consent for inclusion in the research and for publication of images.
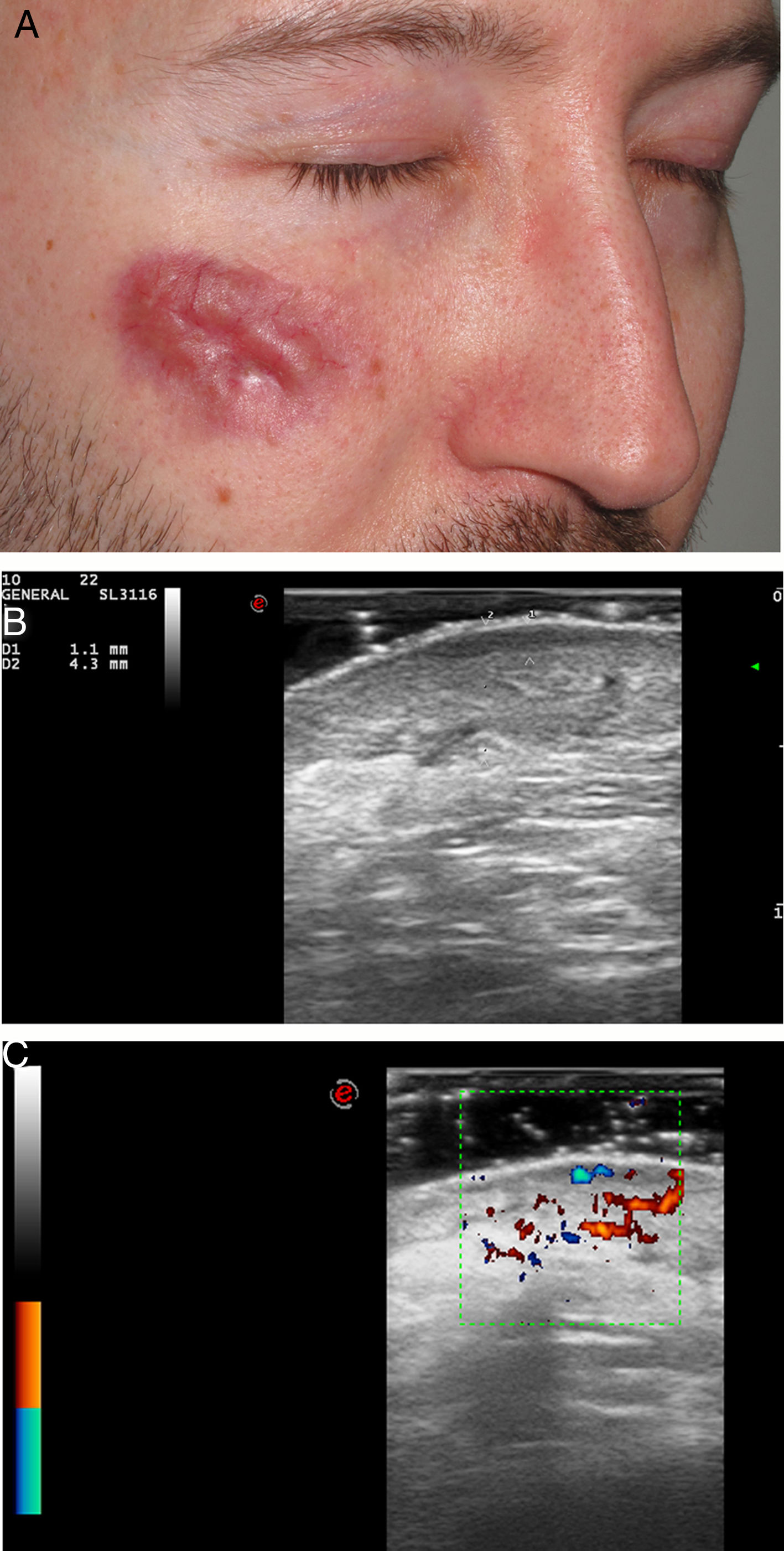
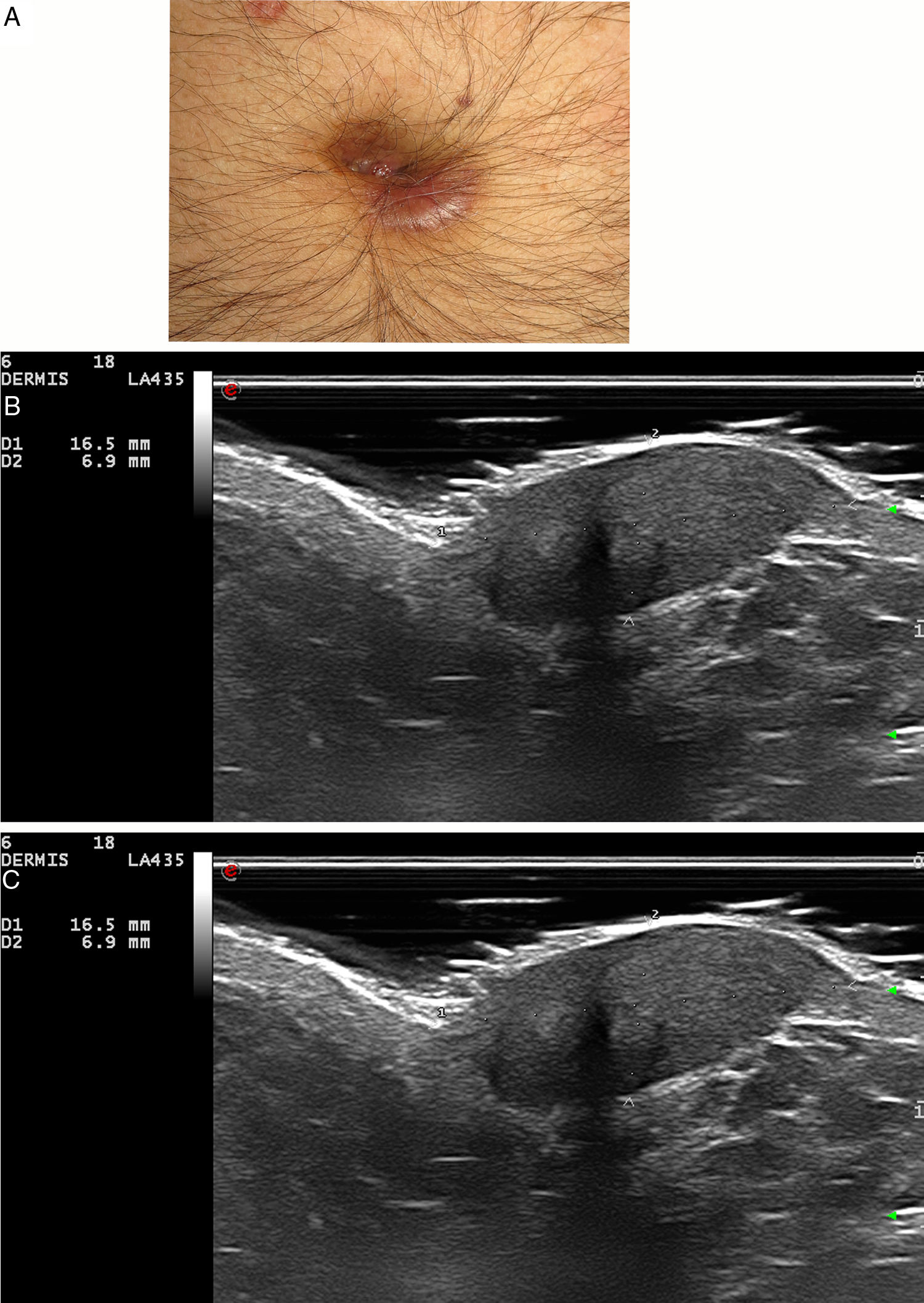
Five patients (six lesions) (four men and one woman) with a median age of 67 years (range, 39-71) and a biopsy-proven GF were included. In three of patients the lesions were located on the face, one on the scalp, one on the ear and one on the umbilicus. Most patients had undergone several treatments without clinical improvement (Table 1). On ultrasonographic evaluation, GF presented in all patients as a hypoechoic and heterogeneous lesion in dermis and hypodermis with an increased vascularity on color Doppler mode (Fig. 1–2). Almost all lesions (5/6) were ill-defined. In 5/6 GF a marked subepidermal hypoechoic/anechoic band was observed. One lesion (case 5, nose) presented a posterior enhancement. There were no significant differences in ultrasound characteristics between facial and extrafacial GF (Table 1).
Characteristics of patients with granuloma faciale.
| Case n | Sex/age (years) | Time of evolution (years) | Anatomic location | Previous treatments | Histological description | Ultrasound features (B-mode ) | Doppler mode |
|---|---|---|---|---|---|---|---|
| 1 | m/39 | 5 | right cheek | topical corticosteroids, hydroxycloroquine, dapsone, laser, topical tacrolimus | Presence of Grenz zone. Dense inflammatory infiltrate constituted mainly by eosinophils, few histiocytes, lymphocytes and occasional plasma cells. | Hypoechoic, heterogeneous and ill-defined lesion in dermis and hypodermis. | Increased vascularity |
| Subepidermal hypoechoic band | Vessels in dermis up to 0.63 mm in diameter. | ||||||
| 2 | m/59 | 8 | scalp | topical corticosteroids, doxycycline, topical tacrolimus | Presence of Grenz zone. Dense perivascular and perianexial inflammatory infiltrate constituted by histiocytes, lymphocytes, plasma cells and occasional eosinophils. | Hypoechoic, heterogeneous and ill-defined lesion in dermis and hypodermis. | Increased vascularity |
| Subepidermal anechoic band | Vessels in dermis up to 1.4 mm in diameter (PSV 9.2 cm/sec, EDV 2.7 cm/sec). | ||||||
| 3 | m/67 | 12 | Ear | topical and intralesional corticosteroids, topical tacrolimus, hydroxycloroquine | Presence of Grenz zone. Dense lymphoplasmocytic inflammatory infiltrates in dermis. | Hypoechoic, heterogeneous and ill-defined lesion in dermis and hypodermis. | Increased vascularity |
| Vessels in dermis up to 0.8 mm in diameter. | |||||||
| Umbilicus | topical and intralesional corticosteroids, topical tacrolimus, hydroxycloroquine | Presence of Grenz zone. Dense lymphoplasmocytic inflammatory infiltrates in dermis. | Hypoechoic, heterogeneous and well-defined lesion in dermis and hypodermis. | Increased vascularity. | |||
| Subepidermal hypoechoic band | Vessels in dermis up to 1.4 mm in diameter | ||||||
| 4 | f/68 | 1 | nose | none | Presence of Grenz zone. Perivascular and interstitial inflammatory infiltrate constituted mainly by histiocytes, neutrophils, eosinophils and occasional plasma cells. | Hypoechoic, heterogeneous and ill-defined lesion in dermis and hypodermis | Increased vascularity. |
| Subepidermal anechoic band | Vessels in dermis up to 0.96 mm in diameter (PSV 17.6 cm/sec, EDV 7.2 cm/sec). | ||||||
| 5 | m/71 | 13 | nose | Imiquimod, cryotherapy | Dense inflammatory infiltrate constituted mainly by eosinophils, histiocytes, neutrophils and plasma cells. Papillary dermal Fibrosis. | Hypoechoic and ill-defined lesion in dermis and hypodermis with posterior enhancement. | Increased vascularity |
| Vesselsin dermis up to 0.66 mm in diameter (PSV 16.3 cm/sec, EDV 5.9 cm/sec). |
m, male; f, female PSV, Peak systolic velocity; EDV, end-diastolic velocity.
Diagnosis of erythematous skin lesions occurring on the face can be challenging. GF can be a highly disfiguring pathology, and it is essential to perform the differential diagnosis with dermatosis of similar clinical appearance, but different treatment such as sarcoidosis, lupus vulgaris, rosacea, fungal infection, mycobacteriosis, discoid lupus erythematosus, adverse reactions to fillers, cutaneous lymphomas and pseudolymphomas.1
HRU is a rapid, low-cost and safe technique. It can be used for diagnosis, follow-up, monitoring response to treatment and to guide interventional procedures in dermatology.4 Literature about ultrasonographic features of facial dermatoses is scarce. We have not found previous reports of ultrasonographic descriptions of GF. In our study facial and extrafacial granuloma faciale presented in most cases as a hypoechoic, heterogenous and ill-defined lesion on dermis and hypodermis with increased vascularity on ultrasound examination. A marked subepidermal hypoechoic band was also found in almost all cases, and it may be secondary to cutaneous inflammation, to the presence of a Grenz zone on histopathology (a characteristic histopathologic feature of GF5) or to photo-ageing, as most lesions were located on sun-exposed skin. Sonographic characteristics may allow to differentiate GF from subacute cutaneous lupus erythematosus as the latter shows thickening and hypoechogenicity of the dermis with a plateau shape, and increased echogenicity of the upper hypodermis with a “foggy appearence”,6 and from inflammatory complications of cosmetical fillers, where the patient is occasionally reluctant to admit the procedure, such as hyaluronic acid and pure silicone (anechoic pseudocysts), liquid silicone (snowstorm appearance), polymethylmethacrylate and calcium hydroxyapatite (hyperechoic dots and bands, respectively).7 Also, HRU may help to differentiate GF from primary cutaneous lymphomas (PCLs) occurring on the face such as primary cutaneous CD4+ small/medium T cell lymphoproliferative disorder, primary cutaneous anaplastic large cell lymphoma, primary cutaneous marginal zone lymphoma and primary cutaneous follicle center lymphoma, among others. In PCLs HRU reveals thickening of dermis with no evidence of necrosis, calcification or posterior acoustic shadowing. Papules of PCLs are seen as focal infiltrative lesions, whilst nodules are seen as pseudonodules and nodules (more frequently in B cell PCLs), and plaques, as hypoechoic, diffusely infiltrative lesions (more predominant in T cell PCLs). On colour Doppler mode, PCLs show hypervascularity, although initial focal infiltrative lesions may be avascular.8
Clinical and histopathological diagnosis of GF may be challenging. We believe that knowing the sonographic characteristics of GF may help in the diagnosis of this disease. Further studies describing ultrasonographic features of inflammatory dermatoses of the face are required.
Conflicts of interestThe authors have nothing to disclose.
Please cite this article as: Morgado-Carrasco D, Giavedoni P, Mascaró JM, Iranzo P. Características ecográficas del granuloma facial y extrafacial. Una serie de casos. Actas Dermosifiliogr. 2021;112:559–563.


