





A 60-year-old man with a history of non–insulin-dependent diabetes mellitus and dyslipidemia consulted us for an asymptomatic lesion on his tongue. He reported that it had been present for approximately 2 years, growing at first but then becoming stable over the past few months.
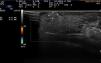
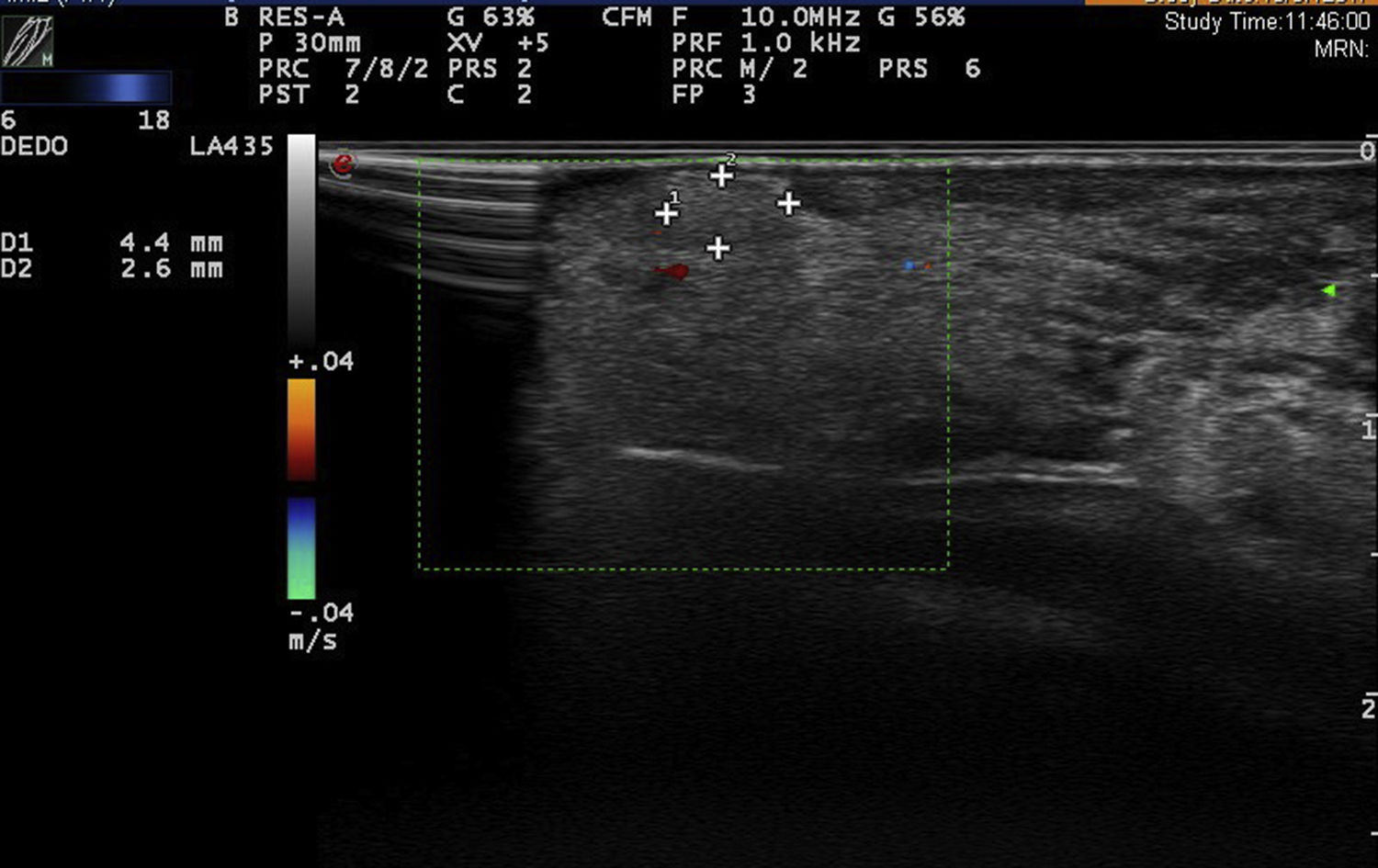
Physical examination showed a rounded well-defined nodule on the right side of the anterior third portion of the tongue. The yellowish nodule measured approximately 6mm at the longest axis, was reddish on the surface, flexible to the touch, and not adherent to deep layers. Dermatologic ultrasound with an 18MHz probe showed an oval tumor that was slightly more hypoechoic than the adjacent tissues. The well-defined but not encapsulated tumor measured 7.5×2.5mm on ultrasound and had no Doppler flow either on the surface or at the center. Fig. 1 shows the full length of the nodule. Suspecting a benign, avascular tumor, we performed a 4-mm punch biopsy. The histopathologic findings showed a proliferation of mature adipocytes distributed in small lobules separated by thin fibrous septa surrounded by normal stroma (Fig. 2). Our diagnosis based on these findings was lipoma of the tongue.
After the biopsy, 2.5mm of the lesion remained (Fig. 3). As the lesion was benign and asymptomatic, we were guided by the patient's preference and chose to wait and watch for changes.

Lipomas are benign neoplasms composed of mature adipocytes that are often found on the arms, legs, trunk and even the face. Lipomas inside the mouth, however, are exceptional, accounting for hardly 1% to 4% of benign lesions. The tongue is the most common oral location, accounting for around 30% in the mouth, and most tongue lipomas occur in the anterior third of the structure and on the side. Other more unusual locations are the buccal mucosa, the lips, or the palate.1,2
Lipomas usually present after the age of 40 years as solitary, well-defined, spherical lesions that do not adhere to base layers. They can be yellowish, especially if superficial. Rarely do they cause symptoms other than local irritation or, if they grow large, problems with chewing; however, these oral lesions rarely exceed 2cm3.
Differential diagnoses should include other lesions of the tongue, such as mucoceles, fibromas, dermoid cysts, salivary gland tumors, lymphangiomas, hemangiomas, neuromas, neurofibromas, schwannomas, adenocarcinomas, ectopic thyroid tissue, or thyroglossal duct remnants.3,4
Many of the aforementioned lesions are similar in clinical appearance and can only be differentiated by means of histologic evaluation. Traditional imaging techniques (simple x-rays, computed tomography scans, magnetic resonance) are often altered by dental implants or fillings. Tongue lesions are therefore frequently removed on the basis of the findings of physical examination alone.5
The generalized use of dermatologic ultrasound in the last 10years has included the inspection of mucosal tissues, but few cases extending this application have been reported in dermatology journals. All such descriptions available have been published in journals of oral medicine or maxillofacial surgery. The lesions described are usually oval, well-defined but not encapsulated, and heteroechoic (iso- or hypoechoic with respect to surrounding structures). They have absent or very weak Doppler signals (Table 1). There might be slight posterior acoustic enhancement. Short, parallel hyperechoic bands are less often seen in these lipomas than in those at other locations.2,5
Principal Ultrasound Findings in the Most Common Tongue Lesions
| Lesion | Morphology | Ultrasound Characteristics | Compressibility | Doppler Flow |
|---|---|---|---|---|
| Lipoma | Round or oval, well defined | Hypoechoic; on occasion, short parallel hyperechoic bands | Yes | Absent, scant |
| Cyst | Round or oval, well defined | Encapsulated, anechoic, posterior enhancement | Partial | No |
| Neurofibroma | Oval, well defined | Hypoechoic and heteroechoic; on occasion, posterior enhancement | No | May have an augmented center and/or perimeter |
| Lymphangioma | Oval, well defined | Encapsulated, alternating anechoic and hypoechoic areas separated by hyperechoic septa | Yes | Scant |
| Hemangioma | Irregular, well defined | Hyperechoic, alternating anechoic and hypoechoic areas separated by hyperechoic septa; on occasion, hyperechoic calcifications with slight posterior acoustic enhancement | Yes | Anechoic spaces, which fill on Doppler imaging |
| Pyogenic granuloma | Irregular, poorly defined, not encapsulated | Hypoechoic and heteroechoic; on occasion, posterior enhancement | No or partial | Augmented |
A lesion on the tongue is examined in much the same way as lesions elsewhere. The anterior two-thirds of the tongue can usually be examined without assistance, but given the limited space in the mouth it may be useful to use a smaller or “hockey-stick” probe to facilitate mobility. A protective shield is necessary when examining mucosal tissue, and the patient should be informed that the gel used for dermatologic ultrasound is nontoxic.
Ultrasound imaging can help the dermatologist evaluate a lesion's size, shape, degree of vascularization, and attachment to other structures and should be considered for the differential diagnosis of tongue lesions.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Ruiz-Rivero J, Echeverría-García B, Tardío JC, Borbujo J. Características ecográficas de los lipomas linguales. Actas Dermosifiliogr. 2019;110:405–407.


