




A 40-year-old patient with no remarkable past history presented with a light brown macule with irregular contours and a diameter of 3cm×4cm on the inner aspect of the right hallux (Figs. 1 and 2). It was asymptomatic and had been present for 6 months.
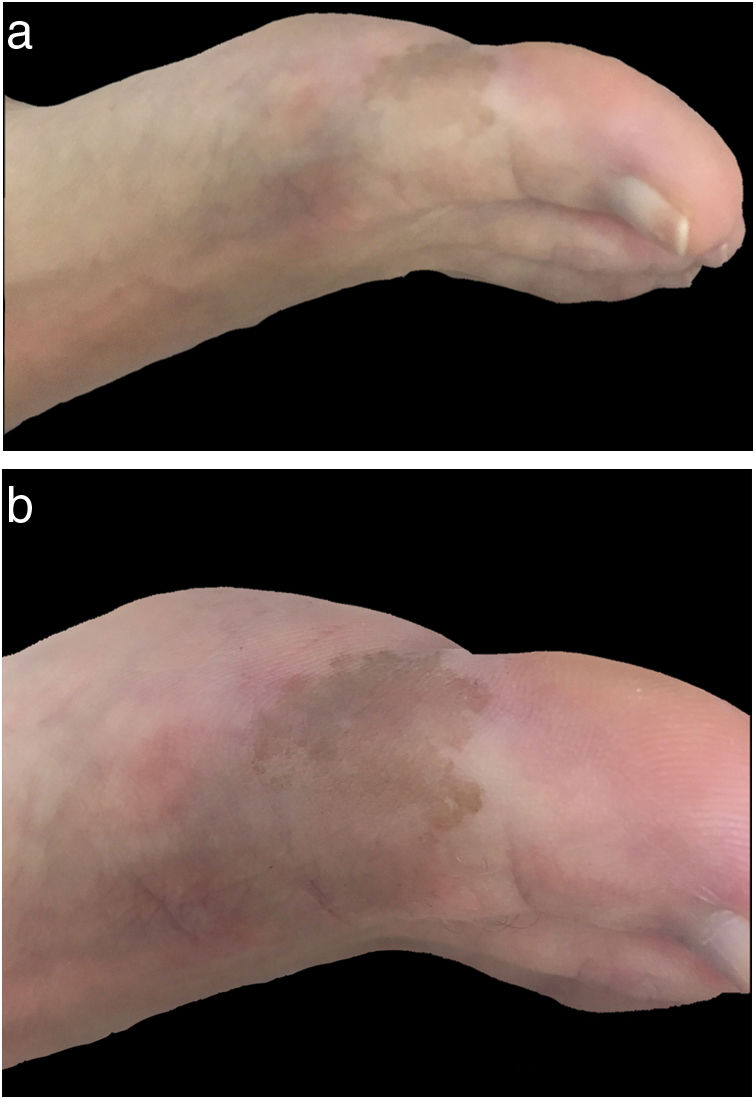
Tinea nigra.
CommentTinea nigra is a superficial mycosis caused by Hortaea werneckii. It is endemic to tropical and subtropical countries and mainly affects children and young adults. Clinically, it presents as a unilateral brown macule with irregular, well-circumscribed contours, predominantly affecting the palmoplantar region. It follows an asymptomatic, chronic course and may be confused with melanocytic lesions.1
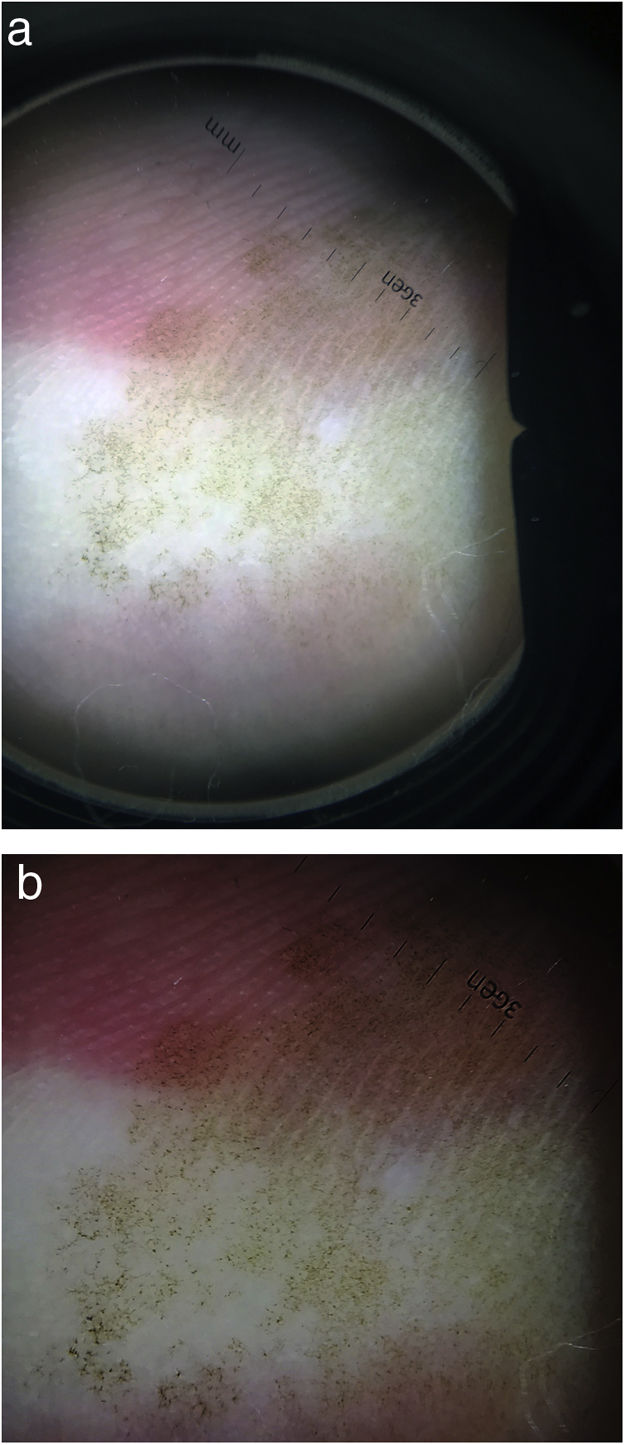
The dermoscopic characteristics of tinea nigra were described by Gupta et al.2 in 1997 as “pigmented spicules” forming a reticular pattern; other findings included fine dots and wispy brownish strands not following the ridges or furrows of the skin. These strands and pigmented spicules correspond to pigmented hyphae in the stratum corneum.3
Noguchi et al.2 later described a case of tinea nigra in which dermoscopy showed a parallel ridge pattern similar to that observed in acral melanoma.
Potassium hydroxide examination is thus recommended to confirm the presence of a superficial mycosis when a parallel ridge pattern is observed in a patient with suspected tinea nigra.
In conclusion, dermoscopy is a valuable tool for evaluating pigmented lesions as it significantly increases diagnostic sensitivity and specificity.
Based on the literature and our experience, we recommend potassium hydroxide examination of pigmented acral lesions with a parallel ridge pattern on dermoscopy to confirm the presence of tinea nigra and avoid unnecessary invasive procedures such as biopsy.4
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Label A, Sole JJ, Larralde M. Dermatoscopia de tinea nigra. Actas Dermosifiliogr. 2021;112:539–540.


