





The trapdoor effect is a possible complication in flap reconstructions, particularly those involving the face. It consists of a bulging, elevated deformity that appears 3 weeks after the intervention. To date there has been no consensus on how the trapdoor effect should be treated. The aim of this article is to report on our experience with this defect and describe how we use the ‘super shaving’ technique to resolve the trapdoor effect in nasal flaps.
Material and methodsWe performed a retrospective, descriptive study of 10 patients who developed a bulging deformity of a nasal flap that was treated surgically with the super shaving technique. We also report on postoperative management.
ResultsThe median age of the 10 patients was 67.7 years and they all developed a bulging transposition flap in the nasal area after conventional or Mohs micrographic surgery. The complication occurred approximately 5 weeks after surgery and healing time was 4 weeks. There were no major postoperative complications and the outcome was of low aesthetic significance compared with the bulging flap. All the patients stated they were very satisfied with the aesthetic outcome.
ConclusionsIn our opinion, the super shaving technique is a fast, effective, simple, and cheap outpatient procedure that offers excellent aesthetic results.
El efecto en trampilla o trapdoor es una complicación posible en un colgajo cuando se utiliza especialmente en la zona facial. Consta de una deformidad elevada y abultada, que comienza 3 semanas después de la intervención, y hasta la fecha no existe consenso en su tratamiento. Es por ello que presentamos nuestra experiencia en esta afección, destacando la técnica de afeitado profundo o super shaving para la resolución del efecto en trampilla de colgajos nasales.
Materiales y métodosEstudio retrospectivo y descriptivo de 10 pacientes que desarrollaron un abultamiento posterior a un cierre mediante colgajo en la zona nasal, que fueron resueltos quirúrgicamente a través de la técnica de super shaving y su manejo postoperatorio.
ResultadosLa edad mediana de los 10 pacientes operados fue 67,7 años, y todos ellos presentaron abultamiento de colgajo de trasposición del área nasal, posterior a una cirugía micrográfica de Mohs o cirugía convencional. El tiempo de aparición de la complicación fue de aproximadamente 5 semanas, y el de cicatrización fue de 4 semanas. Ningún paciente presentó complicaciones mayores en el postoperatorio, y la cicatriz tuvo una incidencia estética baja comparada con el abultamiento. Todos los pacientes refirieron estar muy satisfechos con el resultado estético.
ConclusionesConsideramos que la técnica de super shaving es rápida, efectiva, simple, de bajo costo, se practica de manera ambulatoria, y ofrece resultados estéticamente excelentes para resolver este defecto.
The nose is the most frequent site of the body for nonmelanoma skin cancers (NMSCs), whether basal cell cancer (BCC) or squamous cell cancer (SCC). In the case of BCC, 90% of tumors are located on the head and neck and 25% of those in the nasal region. Similarly, 96% of SCC occur on the head and neck and 20% of those in the nasal region.1,2
Of the approaches for treatment of NMSC in the nasal region, the advantages of surgical excision exceed those of curettage, electrocoagulation, and radiotherapy.1 If direct wound closure is not possible after excision, available options include healing by secondary intention, skin grafts, and local flaps, with those derived from the immediate vicinity being the most desirable as good outcomes are achieved both in functional and aesthetic terms.3,4
Possible immediate postoperative complications of flaps are those inherent to all surgery; ecchymosis, hematomas, dehiscence, partial or total flap necrosis, edema, swelling, and infection.4
The trapdoor defect refers to when a raised and bulging deformity of the tissue occurs within the borders of a semicircular or circular scar. The defect is often observed with transposition flaps, particularly in the nasolabial site.5
This complication was described by Mustarde as a pin cushion defect that usually appears 3 weeks after the procedure, although onset can be as late as 6 to 8 months, with cosmetic impact.5–7 Although the causes have not been determined, it is thought that lymphatic or venous obstruction, excess adipose tissue, beveled wound edges, and hypertrophy or contracture of the scar are implicated in the development of this defect.5 Clodius7 recently defined the defect as a lymphatic abnormality of facial defect reconstruction with flaps. Blood vessel anastomoses precede those of lymphatic anastomoses, and so overload of postcapillary venules usually occurs with increased capillary filtration. Scar formation further hinders the development of the vascular and lymphatic network.8
To date, there is no consensus on the treatment of choice, although corticosteroid injections may limit the formation of the trapdoor defect. One of the techniques commonly used to reduce bulging is lifting the flap, but even then, bulging may persist.9 In those patients in whom this complication is still present, multiple Z-plasties can be performed to attempt to improve the defect.5,10 The combination of scar excision, compression, and immobilization can improve appearance, although these procedures are tiresome for the patients and do not provide a satisfactory solution.7 The trapdoor effect can be prevented or minimized by peripheral undermining of the recipient site of the flap to reduce tension,5 or by straightening the incisions to create a right angle instead of the normally rounded border. Flaps with straight borders instead of curved ones can avoid circular scar contracture.11
We report experience and treatment in patients who develop bulging after flap closure in the nasal area. The complication was resolved with the super shaving approach (term coined by Dr. Ival Peres Rosa).
Material and MethodsPatient SelectionThis was a descriptive, observational, retrospective study of patients who presented with the trapdoor defect in the area of a facial flap as a postoperative complication.
The cases corresponded to operations performed in the Surgery Unit of the Dermatology Department of the Hospital de Clínicas Dr. Manuel Quintela, in Montevideo, Uruguay, and in the Cosmetics, Surgery, and Oncology Unit of the Dermatology Department of the Universidad Federal de San Pablo, San Pablo, Brazil, between January 2015 and January 2018. Review of the medical records and imaging studies and photographs were assessed to derive the following information: age, sex, type of tumor requiring surgery, type of repair used for surgical closure, site of the scar, time until onset of the trapdoor effect, and time to healing after repair. In accordance with departmental protocols, before surgical intervention, patients signed the informed consent for performing surgery and use of photographs in scientific publications. Records from the follow-up visits at 24h, 1 week, and then monthly until wound closure were obtained. To assess the degree of satisfaction with the aesthetic outcome, each patient was asked, on a scale of 1 to 10, the degree of satisfaction obtained with this surgical technique, with 1 being “very unsatisfied” and 10 being “very satisfied.”
Surgical TechniqueCorrection was performed in the dermatology procedure room in an aseptic environment with infiltration of local anesthetic (lidocaine 2%) and epinephrine 1:80 000, and placement of sterile drapes. With one half of a razor blade, the bulging part is shaved, even reaching subcutaneous cell tissue; the surrounding tissue is then leveled with 150 grit wet/dry sandpaper embedded in saline solution.
Essentially, in most cases, shaving completely removes the epidermis and dermis, exposing the subcutaneous tissue. With subsequent abrasion, we correct irregularities resulting from the shaving. Hemostasis is achieved by manual compression; a low-power electric scalpel may be used if necessary. Finally, local dressing is applied with compressive gauze and mupirocin ointment (Fig. 1).

Super shaving technique. A, We can see the trapdoor defect as a complication of transposition pedicle flap closure. B, With one half of a razor blade, the entire bulging part is shaved. C, The surrounding tissue is leveled with 150 grit wet/dry sandpaper embedded in saline solution. D, The outcome on finishing the procedure is shown.
After 24hours, the dressing is changed; strict sun protection is then indicated to avoid hyperpigmentation then until reepilization has occurred (after approximately 15 days). Subsequently, control visits occur at 1 month and 3 months and the wound is photographed.
ResultsThe super shaving technique was performed in 10 patients with bulging flap (Table 1).
| Patient | Age | Sex | Tumor Excised | Nasal Site | Surgery Performed | Type of Closure | Onset of Trapdoor Defect | Healing Time | Esthetic Outcome |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 60 | M | BCC | Lateral nasal wall | Mohs surgery | Transposition flap | 4 weeks | 4 weeks | 10 |
| 2 | 51 | F | BCC | Nasal dorsum | Mohs surgery | Transposition flap | 12 weeks | 4 weeks | 10 |
| 3 | 64 | F | BCC | Nasal dorsum | Mohs surgery | Transposition flap | 4 weeks | 4 weeks | 10 |
| 4 | 76 | M | BCC | Dorsum and left nasal ala | Mohs surgery | Transposition pedicle flap | 8 weeks | 4 weeks | 10 |
| 5 | 74 | M | BCC | Nasal dorsum | Mohs surgery | Transposition flap | 4 weeks | 4 weeks | 10 |
| 6 | 75 | F | BCC | Nasal ala | Conventional surgery | Transposition flap | 5 weeks | 6 weeks | 10 |
| 7 | 47 | M | BCC | Nasal ala | Conventional surgery | Transposition flap | 5 weeks | 3 weeks | 10 |
| 8 | 71 | M | BCC | Nasal ala | Conventional surgery | Transposition flap | 6 weeks | 5 weeks | 10 |
| 9 | 63 | F | BCC | Nasal ala | Conventional surgery | Transposition flap | 6 weeks | 4 weeks | 10 |
| 10 | 74 | M | SSC | Nasal dorsum | Mohs surgery | Transposition flap | 5 weeks | 4 weeks | 10 |
The median age of the patients was 67.5 years (51 to 76 years); 6 were men and 4 were women.
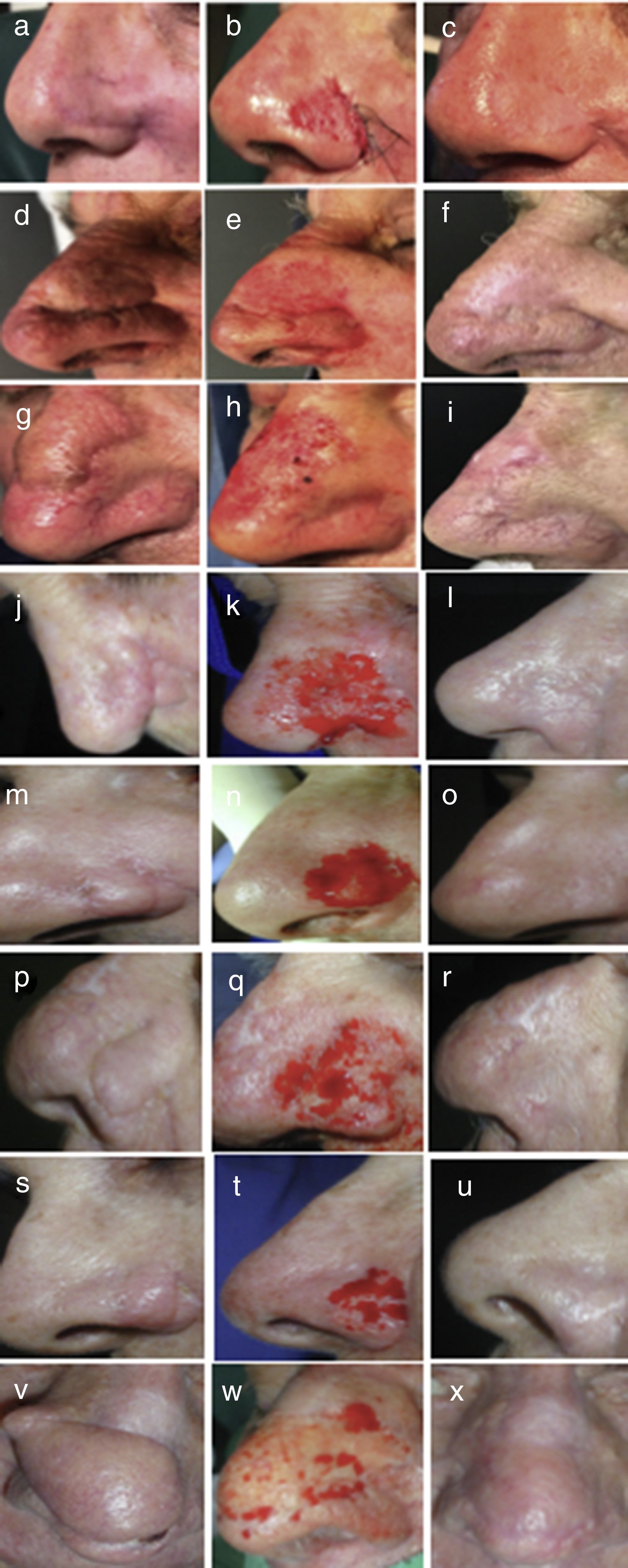
The trapdoor defect was the result of closure of surgical defects by transposition flap in 9 patients with BCC and 1 patient with SCC, mainly in the nasal area. The Mohs micrographic procedure was used in 6 and conventional surgery in 4. In all 10 cases, a transposition flap was used for closure (Fig. 2).
After reconstruction, the median time to onset of trapdoor defect was 5 weeks (4 to 12 weeks).
After performing the super shaving technique, complete wound closure was observed at 4 weeks (3 to 4 weeks).
The mean degree of satisfaction with the aesthetic result was 10 (highly satisfied) in the follow-up visit on discharge of the 10 patients who had undergone the procedure.
No relapses were reported in the trapdoor defect during follow-up of these patients.
DiscussionDifferent treatments are available for the trapdoor defect, including manual lymphatic drainage (MLD), intralesional corticosteroids, and complex postoperative procedures.5,9,12 Although MLD leads to a cosmetic improvement in the trapdoor defect, the procedure requires that the patient attend the clinic for 30-minute sessions 3 times a week for at least 1 month.12 Intralesional corticosteroids can be successful in mild trapdoor defects.9 In general, triamcinolone acetonide is used at an initial concentration of between 20mg/mL and 40mg/mL at a dose of 0.4 to 0.8mL once a week, separated by intervals of 3 to 4 weeks.5 In cases of more significant deformity, surgical correction is necessary to redirect the contractile forces of the scar and break the contractile ring; for this purpose, Z-plasties can be used alone or in combination with extensive tissue undermining.10 However, sometimes, complete resolution cannot be achieved given the extent of curvature; the greater the curvature the higher the contractile forces.5
In the series of cases of super shaving reported here, our intent is to present this novel technique with excellent aesthetic outcomes as an option for this complication.
As described in the literature, the trapdoor defect can present from 3 weeks onwards and sometimes as late as 8 months; in our patients, presentation was early, before 3 months after reconstruction following Mohs micrographic surgery or conventional surgery.5,6 In addition, the fact that the surgery involved the nasal or perinasal area was a risk factor for lymphedema,11 and this was observed in our patients given that the scars were circular or semicircular.5
Of note is that although our patients attended subsequent follow-up visits to assess wound healing, they continued in follow-up with dermatology because of cutaneous carcinoma.
With regards the final aesthetic outcome, all our patients were satisfied with the aesthetic result after the swelling had resolved. As a side effect of the technique, we should mention the possibility of leaving a scar. This occurred in few patients and when scarring did occur, the overall aesthetic impact was lower than bulging (Fig. 2l and x).
In the present study, we present an effective, simple, inexpensive, outpatient technique with low postoperative burden. Patients can return to normal daily activities quickly and, to date, no complications have been reported. Aesthetic outcomes have been excellent and so this technique should be considered as another option for the treatment of trapdoor defect.
The main limitation of our study is the small number of patients included and the limited follow-up duration. Longer follow-up is necessary to assess the future complications of the super shaving technique.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Correa J, Magliano J, Peres I, Bazzano C. The Super Shaving Technique to Correct the Trapdoor Effect in Nasal Flaps. Actas Dermosifiliogr. 2019;110:33–37.


