



Reconstruction after surgery for periorbital tumor lesions can give rise to cicatricial ectropion if there is excessive vertical tension after reconstruction. Furthermore, the risk of eversion of the eyelid margin is enhanced by excess laxity in elderly individuals in whom tumors are also more prevalent.
Appropriate eyelid examination before surgery can enable the most appropriate repair technique to be designed and so minimize the risk of ectropion. Should postoperative ectropion occur, repair can be performed by canthal resuspension or horizontal shortening of the lower eyelid.
One of the most widely used techniques to achieve both resuspension of the external canthus and eyelid shortening is the tarsal strip technique.1 Alternatively, ectropion can be repaired by canthopexy (attaching the lateral canthal tendon to the orbital rim without the need for canthotomy). Flaps (such as the Tripier flap), grafts, or synthetic material can be used with both techniques to provide bulk to the lower eyelid in the event that ectropion is due to loss of volume.
We describe, with a surgical video, postoperative ectropion repair with a tarsal strip (Fig. 1) (video in supplemental web material).
Description of the Technique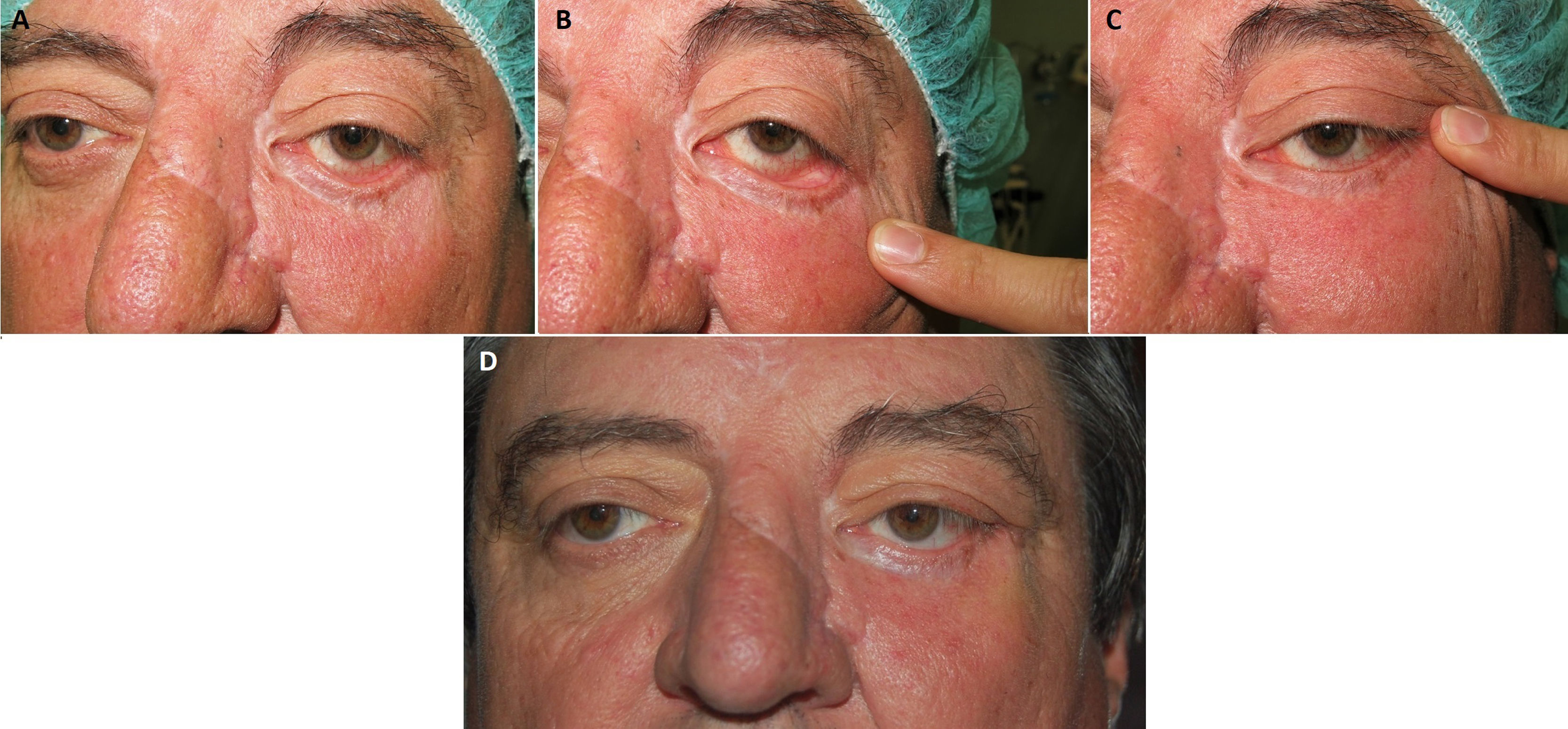
The patient was a 56-year-old man with postoperative cicatricial ectropion and extensive external canthal laxity (Figs. 1A-C). Faced with predominance of the lateral component (hyperlax lateral canthal tendon), it was decided to perform canthoplasty with a tarsal strip.
The tarsal strip procedure starts under local anesthetic, with an incision of 1 cm in the skin and orbicularis muscle of the external canthus and cantholysis (opening the lateral canthal angle).1–3
Then the free margin of the tarsus inferior is released in the form of a strip by making an infracilary incision. Once this incision is made, mobility is checked (lateral advancement) and the eyelid positioning is confirmed, paying attention to the amount of tissue of the strip that is to be anchored as this has to be de-epithelized.
Once shaped and de-epithelized, one end is anchored to the periosteum of the orbital rim with resorbable 5/0 stitches to form a neocanthus. The anchor point for the canthal repositioning is level with the periosteum, in the internal face of the lateral orbital rim, 2 mm above the medial canthus, to ensure appropriate lubrication (the tears follow a superolateral or inferomedial pathway).
Finally, the initial incision in the anterior lamella is sutured with simple continuous stitching with resorbable 5/0 thread.
Indications- •
Canthal malposition1,2
- •
Paralytic ectropion1,2
- •
Involutional ectropion: horizontal eyelid laxity or canthal laxity1,2
- •
Postoperative ectropion
Thus, tarsal strip canthoplasty can be used in the prevention of ectropion in patients with horizontal eyelid laxity who will undergo tumor excision and when tension in the lower eyelid is anticipated; in the repair of postoperative cicatricial and involutional ectropion, potentially in combination with other techniques (Z-plasty or tissue repositioning by flap advancement, grafting, or synthetic material) and in the repair of involutional ectropion with moderate/severe laxity in which canthopexy is not sufficient.1,3
ContraindicationsThere is no absolute contraindication. Coagulation disorders that might cause severe bruising and compromise intraocular pressure could be considered contraindications.
Complications- •
Eyelid edema
- •
Ecchymosis/periorbital hematoma
- •
Chemosis of the conjunctiva
- •
Conjunctivitis
- •
Blepharitis
- •
Eversion of the lacrimal punctum and epiphora
- •
Trichiasis
- •
Suture dehiscence
- •
Granuloma associated with suture reaction
Lateral tarsal strip canthoplasty is a simple and effective technique for moderate-severe postoperative or involutional ectropion.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Fernández Canga P, Varas-Meis E, Rodríguez Prieto MA. Reparación de ectropión posquirúrgico mediante tira tarsal. Actas Dermosifiliogr. 2021;112:269–270.


