




The schwannoma, neurilemmoma, or neurinoma is a benign tumor that arises from the Schwann cells of the cranial and peripheral nerves. It appears in individuals between 20 and 50 years of age and is equally common in men and women.1
Schwannomas are usually sporadic, but in some cases they are associated with neurofibromatosis type II, schwannomatosis, Carney complex, or, more rarely, with radiation therapy, with a latency of up to 50 years (acoustic schwannomas).2
Around 25% of extracranial schwannomas arise on the head and neck, and approximately 1% are intraoral.3,4
Our patient was an otherwise healthy man of 52 years of age, with no past medical history of interest. He presented a single tumor that had appeared 18 months earlier on the dorsum of tongue. The tumor was occasionally painful. There was no history of surgery or trauma to the area. Physical examination revealed a nodule of 2mm diameter on the dorsum of the tongue. The lesion was slightly erythematous, shiny, well-defined, slightly tender, and had a smooth surface and a rubbery consistency (Fig. 1).

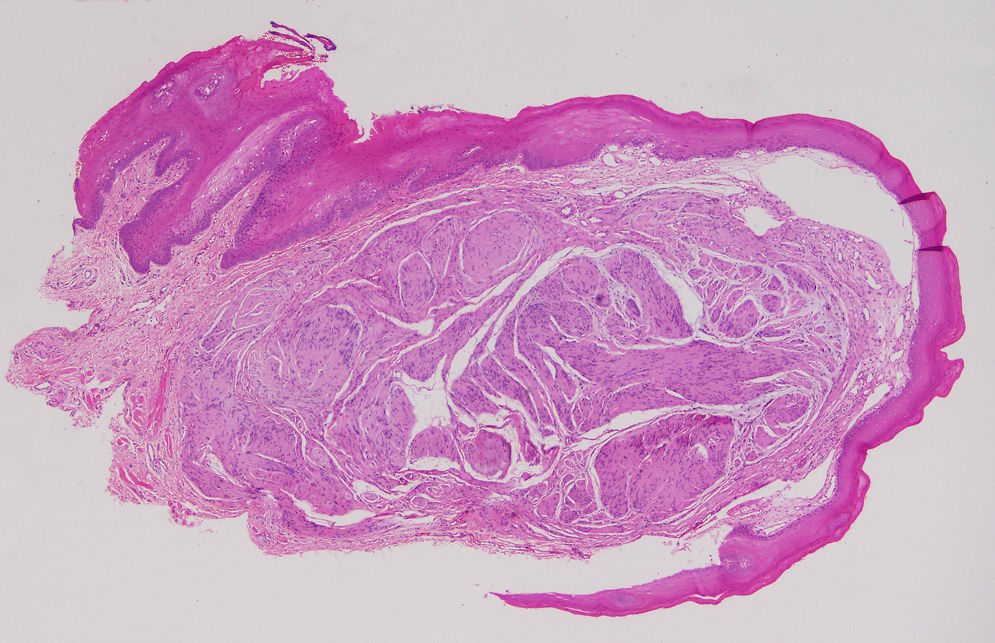
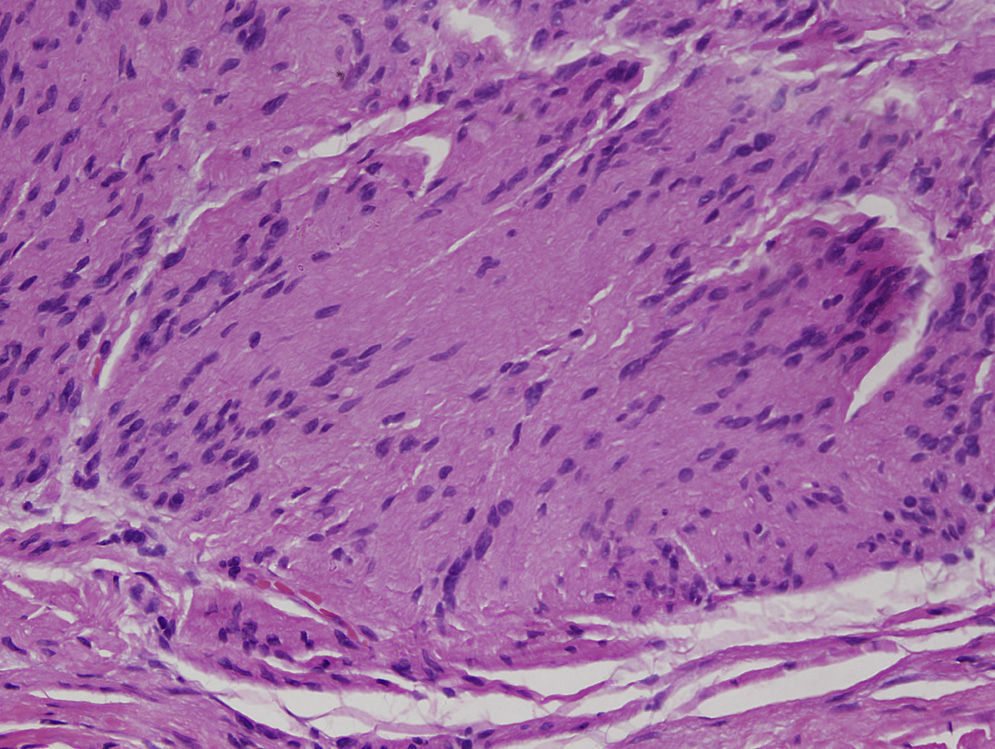
Simple excision of the lesion was performed and histopathology revealed a clearly circumscribed tumor composed of fascicles of spindle-shaped cells, lying beneath the mucosa of the tongue (Fig. 2). At higher magnification, elongated cells were visible; the cells did not show atypia and their nuclei were arranged in line forming the typical “Verocay bodies” (Fig. 3). Immunohistochemistry was positive for S100. A diagnosis of classic schwannoma was made based on these findings.
After excision of the lesion, the wound was closed by direct suture and there have been no surgical complications or recurrence after 6 months of follow-up.
Schwannoma is rare on the tongue. Cohen et al.1 performed a review of schwannomas on the tongue published in journals indexed in PubMed and found 126 cases over a period of 56 years (including 2 cases published in the same article).
Schwannoma presents clinically as a firm, slow-growing tumor that can reach a variable size. Symptoms depend on the site and size, and the tumor can be painful,3 as in the case we have presented, or asymptomatic. When situated on the tongue, some patients describe inflammation, fasciculations, or weight loss associated with difficulty swallowing. Very rarely the lesion can grow rapidly and ulcerate.5
The definitive diagnosis is histological, by observation of a well-defined, encapsulated tumor formed of spindle-shaped cells that can be arranged in 2 patterns. The “Antoni A areas”, which are more cellular and contain the characteristic Verocay bodies, formed of elongated cells with no atypia; the cell nuclei are arranged in line and their cytoplasm is fused into eosinophilic masses. The “Antoni B areas” contain randomly distributed cells in a myxomatous stroma.1–6 Immunohistochemistry is positive for S100. Depending on the morphological variant, schwannomas can be classified into classic, cellular, plexiform, ancient (degenerated), and melanotic.2
Loss of function of the merlin protein (coded by gene NF23) appears to be the cause of the appearance of schwannomas. This protein has complex functions that are essential to various pathways in the nucleus and in the cell membranes. Loss of merlin function in the nucleus leads to an increased expression of membrane proteins, including integrins and growth factor receptors. These growth factors are usually inhibited by cell-cell contact. The absence of merlin favors their activation, stimulating mitogenic and survival pathways and favoring a lack of cell polarization. These alterations cause schwannoma cells to be unable to bind to an axon.2
The clinical differential diagnosis includes those lesions that present as a well-encapsulated tumor: granular cell tumor, salivary gland tumor, leiomyoma, neurofibroma, lymphangioma, hemangioma, cyst, lipoma, and others.
Treatment is surgical and is more complex in those tumors situated on the base of the tongue.6 Malignant change and recurrence are rare.2
We have presented this case as schwannoma is uncommon on the mucosa of the tongue but it is included in the differential diagnosis of benign tumors of the oral mucosa. As occurs with many of these tumors, the final diagnosis is made on histology of the surgical specimen.
Please cite this article as: Feltes-Ochoa RA, Maseda-Pedrero R, Ruíz-Burguillos E. Schwannoma de la lengua. Actas Dermosifiliogr. 2015;106:512–514.


