





Psoriasis is a chronic inflammatory skin disease that typically affects the extremities, trunk, scalp, and nails. Psoriatic cheilitis as an exclusive presentation is very rare,1 and to our knowledge, only 5 cases have been reported to date.2–6 The absence of cutaneous lesions causes diagnostic difficulties that can result in misdiagnosis and inadequate treatment.
We report the cases of 2 young adults who presented with psoriasis of the vermilion of the lips as the only disease manifestation. Response to topical tacrolimus 0.1% treatment was good in both cases.
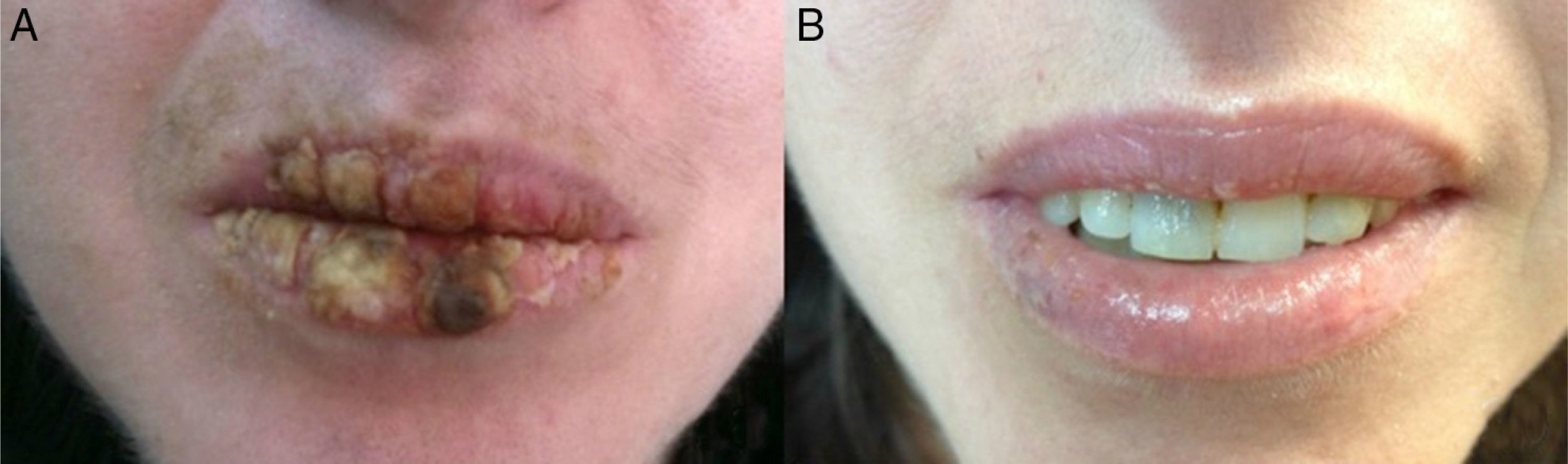
The first case involved a 28-year-old white woman referred to our clinic with a 3-month history of scaly plaques on the vermilion of her lips and a clinical diagnosis of contact cheilitis. Clinical examination revealed an erythematous fissured plaque over the entire upper and lower lip surface, covered by thick white-yellowish scales (Fig. 1A). Full body examination did not reveal any evidence of intraoral or cutaneous involvement. Apart from a 10-year history of Hashimoto thyroiditis, the patient's medical history was unremarkable. However, she did mention that her brother had psoriasis. Contact cheilitis was excluded following negative patch tests. Subsequent biopsy and histological examination confirmed the clinical suspicion of psoriasis. The patient received initial treatment with salicylic acid 5% ointment twice daily for 5 days, followed by a 1-month course of topical tacrolimus 0.1% twice daily, resulting in adequate control of disease activity (Fig. 1B). The patient is currently on maintenance treatment with twice-weekly application of tacrolimus 0.1% ointment.
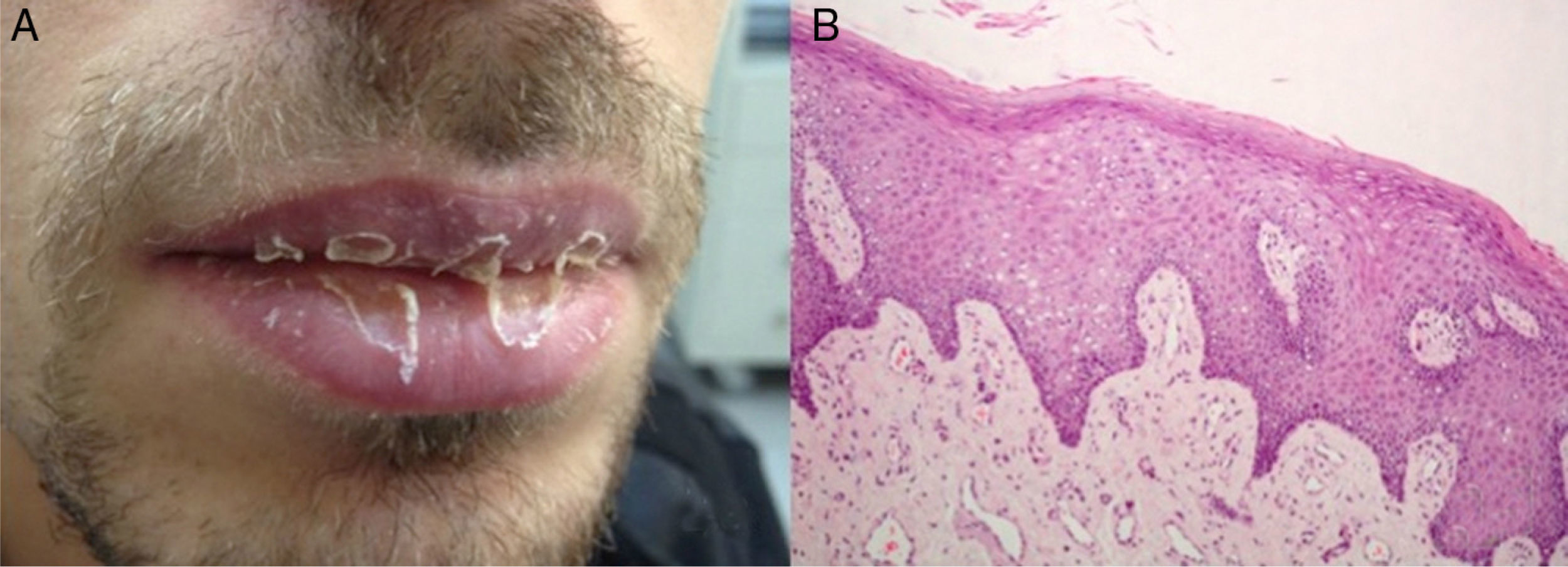
The second case involved a 20-year-old white man referred to our clinic for further assessment of a 2-year history of recurrent erosive cheilitis, characterized by fissures and white-yellowish scales on the vermilion borders of both lips (Fig. 2A). Intraoral and cutaneous lesions were absent. The patient reported exacerbations, particularly during winter. His medical history was unremarkable; there was, however, a positive family history of psoriasis (his mother). After excluding contact cheilitis by patch testing, we performed a lip biopsy. Histopathology showed mounds of parakeratosis and hypogranulosis, acanthosis, and dilated and vertically elongated papillary vessels (Fig. 2B), leading to a diagnosis of psoriatic cheilitis. The patient was started on salicylic acid 5% twice daily for 3 days, followed by topical tacrolimus 0.1% twice daily for the next month. The treatment resulted in the gradual remission of lesions, but discontinuation led to a flare-up, which was managed with the same regimen. To avoid recurrences the patient was advised to use tacrolimus 0.1% twice weekly, with excellent results.
Perioral psoriasis is an unusual presentation of psoriasis. It is clinically characterized by cracking and scaling of the lips and can have a profound emotional, social, and physical impact on patients’ lives.1,4 In the vast majority of the cases, coexistence of typical psoriatic lesions elsewhere on the body facilitates diagnosis. To the best of our knowledge, exclusive lip involvement is very uncommon, with only 5 cases reported in the literature.2–6 In 2 of these cases, involvement of the vermilion of the lips preceded cutaneous manifestations by at least 2 months.5,6 Brenner et al.7 reported a case of psoriatic cheilitis triggered by protruding teeth as a result of Koebner phenomenon; the condition was resolved by replacing the teeth with a nonirritating prosthesis. Table 1 summarizes the main epidemiological and clinical characteristics of all the cases reported to date, including ours. Perioral psoriasis as a single site of involvement can pose significant diagnostic difficulties. Due to a lack of specific diagnostic criteria, it has been suggested that a chronic course, with resistance to treatment and frequent recurrences, should raise the suspicion of psoriatic cheilitis.1 A positive family history and HLA typing have also been described as important in supporting the a diagnosis of perioral psoriasis.
Summary of cases of psoriatic cheilitis reported in the literature.
| Sex | Age, y | Skin lesions at presentation | Oral lesions | Treatment | Outcome | Exclusive lip involvement | |
|---|---|---|---|---|---|---|---|
| Tosti et al.2 | F | 24 | No | No | Steroid cream | CR | Yes |
| Rahman et al.3 | F | 20 | No | No | Triamcinolone acetonide ointment | CR | Yes |
| Sehgal et al.4 | F | 16 | No | No | Tacrolimus+calcipotriol+betamethasone dipropionate | CR | Yes |
| Ersoy-Evans et al.5 | F | 19 | No | No | Fluticasone propionate 0.005% ointment | CR | No |
| Baz et al.6 | F | 22 | No | No | Mometasone furoate 0.1% | CR | No |
| Current cases | M | 20 | No | No | Tacrolimus+salicylic acid | CR | Yes |
| F | 28 | No | No | Tacrolimus+salicylic acid | CR | Yes |
Abbreviations: CR, complete response; F, female; M, male.
Therapeutic modalities such as topical steroids and tacrolimus alone or in combination with calcipotriol have produced adequate response in patients with perioral psoriasis.2–6,8 Tacrolimus, a calcineurin-inhibitor with anti-inflammatory properties, lacks the well-known adverse effects associated with steroids. Yamamoto and Nishioka9 reported a case in which topical tacrolimus ointment was used to treat psoriasis of the vermilion of the lips, with very promising results. Moreover, this treatment combined with salicylic acid gel has been shown to increase the penetration and absorption of the drug, enhancing therapeutic action.10
In conclusion, we have described 2 new cases of psoriatic cheilitis with exclusive lip involvement treated successfully with topical tacrolimus 0.1% in combination with salicylic acid, indicating their possible therapeutic role in this troublesome localization. We suggest that psoriasis should be considered in cases of refractory long-standing eczema-like cheilitis, even in the absence of a positive family or personal history of psoriasis.


