





For many years Grover disease (GD) was classified as an acantholytic and transient dermatosis. It is now known that GD is not necessarily transient1 and can give rise to several different histological patterns in addition to the 4 classical acantholytic patterns (Hailey-Hailey, Darier-like, spongiotic, and pemphigus-like).2,3 Forms of GD with nonclassical histological patterns described in recent years include dysmaturative, lichenoid, vesicular, and porokeratotic forms,2 a lentiginous form,4 and even a pseudoherpetic form.5 A common feature of all these forms is that acantholysis and dyskeratosis may not constitute the main clinical sign, may be focal, or may even be absent,2 complicating histological diagnosis.
Importantly, in most cases these polymorphic histological findings are not associated with major clinical variability. Therefore, correlation of clinical and histological findings is fundamental, especially in early lesions, in order to establish an accurate diagnosis.2,4
Case DescriptionA 53-year-old man with no known underlying disease presented pruritic, papule-like lesions on the upper thorax, axillae (Fig. 1), and pubis that had appeared 10 years earlier. The lesions worsened in response to exposure to heat and sweating.

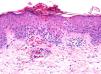
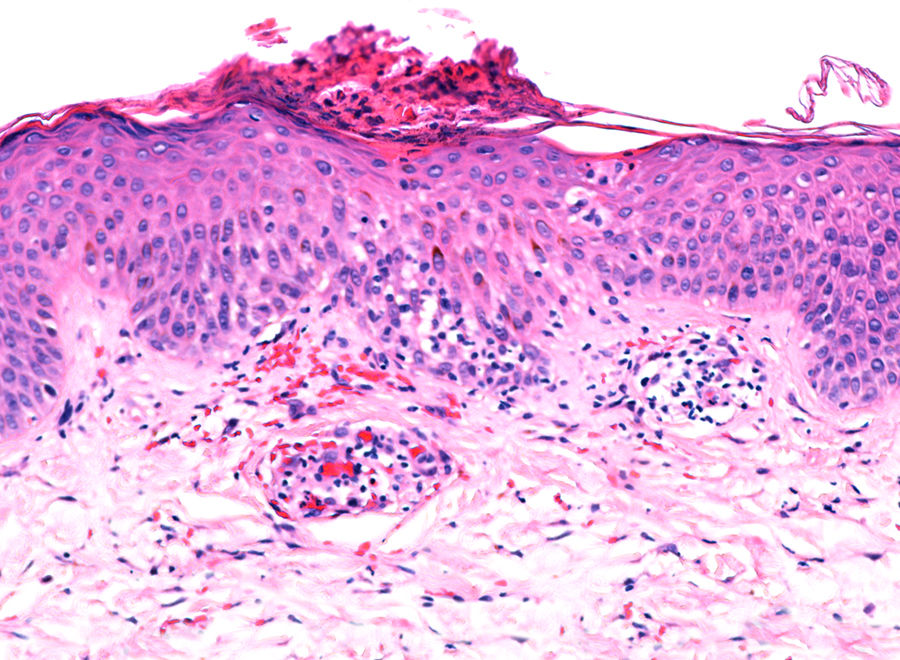
Histology revealed the formation of a cornoid lamella with a column of parakeratosis (Fig. 2), together with spongiosis, focal vacuolar damage, and erythrocyte extravasation (Fig. 3). Nonspecific perivascular inflammatory infiltrate was evident in the dermis. A diagnosis of porokeratosis-like GD was established.
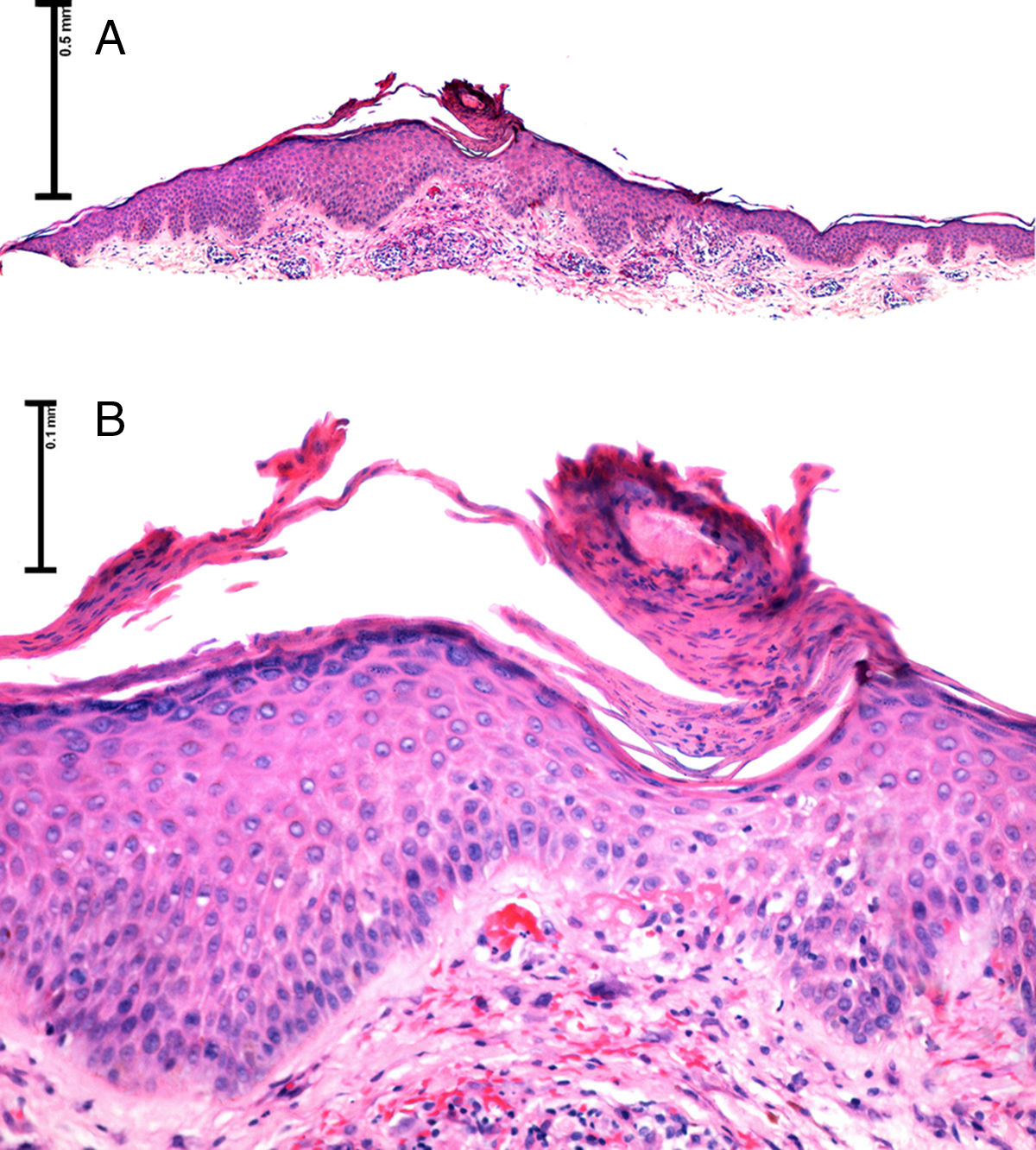
A, Panoramic image showing an oblique layer of parakeratosis on an acanthotic epidermis (hematoxylin-eosin, original magnification×2). B, Enlarged image showing the epidermis with a central depression associated with an oblique column of parakeratosis and hypogranulosis (hematoxylin-eosin, original magnification×4).
GD was first described in 1970, and was associated with 2 distinct histological patterns: Darier-like and Hailey-Hailey-like.6 In 1977, the same author described additional classic acantholytic patterns.7
Subsequent studies investigated the clinical and epidemiological aspects of GD and described discrete clinical forms: transient; persistent, chronic, asymptomatic1; and predominantly seasonal.8 In recent years, the histological characteristics initially proposed by Grover and Park in 19706 have been re-evaluated, and GD is now considered a polymorphic entity for which least 9 histological patterns are described. In their 2010 analysis of 22 cases, Melwani and coworkers described the lentiginous pattern as a diagnostic clue in cases of early GD.4 That same year, a review of 120 cases by Fernández-Figueras and coworkers added 5 histological subtypes to the 4 initially described by Grover et al7: lentiginous, lichenoid, vesicular, dysmaturative, and porokeratotic.2
Fernández-Figueras et al2 described for the first time porokeratotic GD, an infrequent histological form of GD characterized by the formation of a cornoid lamella without epidermal hyperplasia, dyskeratosis, or acantholysis, in some cases associated with spongiosis and basal vacuolar damage, as observed in the present case.
Although parakeratotic columns had been previously described as a feature of Darier-type GD, associated with dyskeratosis, round bodies, and acantholysis,1,7 this finding had not been previously described in isolation. It should be borne in mind that while the presence of parakeratotic columns is a striking histological finding, it is not specific and is observed in several conditions (Table 1).9
Porokeratosis-like GD is a rare entity: it accounted for less than 5% of cases in the case series by Fernández-Figueras et al,2 and few cases are reported in the literature.
These unusual patterns can be difficult to recognize, since the alterations can be subtle, focally distributed, or combined.1,2,4 For example, in our patient we observed areas with a spongiosis-like pattern and vacuolar damage in the basal layer, in addition to the porokeratotic-type pattern (Fig. 3).
The presence of these acantholytic and nonacantholytic patterns suggests that GD is a polymorphic entity that may be frequently underdiagnosed in daily practice.
An interesting aspect of this case is that porokeratosis-like GD is an infrequent histological variant not characterized by the classical dyskeratotic and acantholytic changes.2 The histological heterogeneity of GD has led to its inclusion in the differential diagnosis of multiple entities.1,2
Awareness of the existence of nonclassical histological patterns can help avoid misinterpretation and unnecessary additional biopsies.2 Clinicopathological correlation is essential to establish an accurate diagnosis.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Montoya C, Arias LM, Salazar M, Flórez HA. Enfermedad de Grover tipo poroqueratósico: más allá de un patrón acantolítico. Actas Dermosifiliogr. 2019;110:332–334.


