


Loose anagen hair syndrome (LAHS) is a disorder of abnormal anchorage of the hair. Recently, a couple of trichoscopic signs have been reported in LAHS. We present new trichoscopic findings in 12 children. Dermoscopy can be an additional tool for diagnosing LAHS at the office.
Clinically, hairs can be easily and painlessly pulled from the scalp. It is usually described in blonde girls aged 2–6 years of age who consult for hair thinning and hair that “will not grow”, although this condition has also been described in males and children with darker phototypes too. Common findings in the trichogram are most anagen hairs, ruffled cuticles, and hockey stick-shaped bulbs.1–4 Recently, some trichoscopic signs have been reported in LAHS.5 Herein we describe the clinical and trichoscopic findings in 12 children with LAHS.
We reviewed the clinical and dermoscopic pictures of children with a diagnosis of LAHS confirmed by a trichogram, and performed by a pathologist experienced in hair diseases from 2020 through 2023. The trichoscopic pictures were taken with Fotofinder® or with Dermlite PhotoX® attached to a camera (Fig. 1). Twelve cases of LAHS were found (8 girls and 4 boys) aged 1.5–8 years, including two sets of sisters (Table 1).
, scales (red arrow), cadaveric hair (light green arrow), exclamation hair (yellow arrow), bended hair (white arrow), “dirty dots” (orange arrow), pigmented network (light purple arrow), dystrophic hair (dark green arrow), color dots (red and blue) (dark purple arrow), fragments of hair shaft out of its follicle (yellow rectangle), transverse bright bands (blue rectangle), flame hair (red rectangle), granular rectangular structures (green rectangle), coiled proximal hair (purple rectangle), and perifollicular hyperkeratosis (grey rectangle).")
Trichoscopic findings in patients with LAHS. Vellus hairs (blue arrow), scales (red arrow), cadaveric hair (light green arrow), exclamation hair (yellow arrow), bended hair (white arrow), “dirty dots” (orange arrow), pigmented network (light purple arrow), dystrophic hair (dark green arrow), color dots (red and blue) (dark purple arrow), fragments of hair shaft out of its follicle (yellow rectangle), transverse bright bands (blue rectangle), flame hair (red rectangle), granular rectangular structures (green rectangle), coiled proximal hair (purple rectangle), and perifollicular hyperkeratosis (grey rectangle).
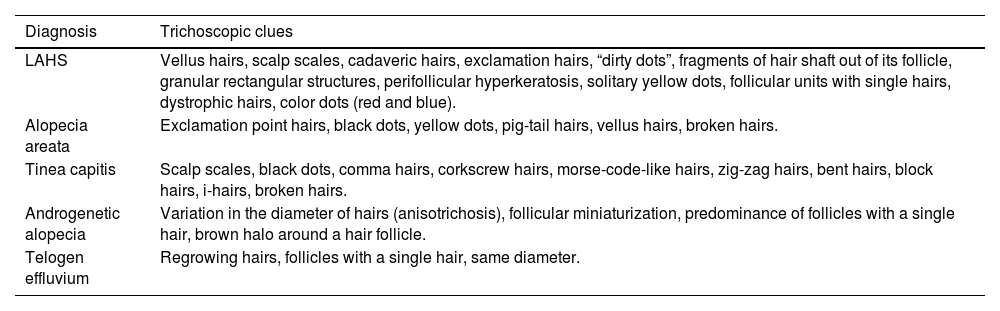
Trichoscopic clues in the differential diagnosis of LAHS.
| Diagnosis | Trichoscopic clues |
|---|---|
| LAHS | Vellus hairs, scalp scales, cadaveric hairs, exclamation hairs, “dirty dots”, fragments of hair shaft out of its follicle, granular rectangular structures, perifollicular hyperkeratosis, solitary yellow dots, follicular units with single hairs, dystrophic hairs, color dots (red and blue). |
| Alopecia areata | Exclamation point hairs, black dots, yellow dots, pig-tail hairs, vellus hairs, broken hairs. |
| Tinea capitis | Scalp scales, black dots, comma hairs, corkscrew hairs, morse-code-like hairs, zig-zag hairs, bent hairs, block hairs, i-hairs, broken hairs. |
| Androgenetic alopecia | Variation in the diameter of hairs (anisotrichosis), follicular miniaturization, predominance of follicles with a single hair, brown halo around a hair follicle. |
| Telogen effluvium | Regrowing hairs, follicles with a single hair, same diameter. |
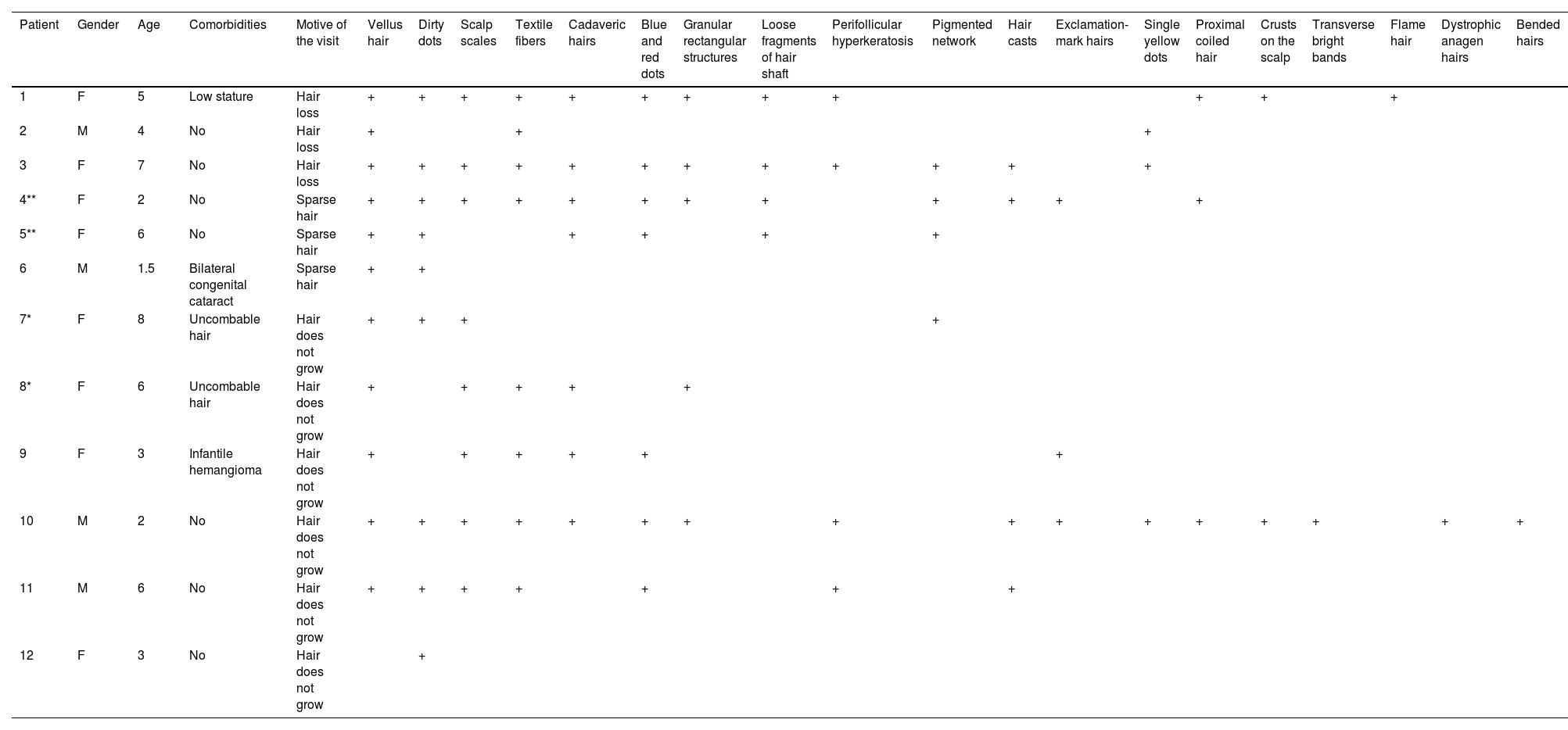
All dermoscopic pictures were analyzed by two dermatologists (AGC and LJPH). The most common trichoscopic findings were vellus and slightly pigmented hairs (11/12), “dirty dots” (9/12), scalp scales (8/12), textile fibers (8/12), cadaveric hairs (7/12), and blue and red dots (7/12) that seem to be caused by an external agent adhering to the skin, such as paper, ink, or paint (Table 1).
Furthermore, we found granular rectangular structures (5/12), loose fragments of hair shaft out of the follicle (4/12), perifollicular hyperkeratosis (4/12), pigmented network on the scalp (4/12), hair casts (4/12), exclamation-mark hairs (3/12), single yellow dots (3/12), and proximal coiled hair (3/12).
In children, trichoscopy is a useful, painless, friendly and widely available diagnostic technique at the dermatology office. The differential diagnosis of LAHS includes alopecia areata (AA), trichotillomania, tinea capitis, androgenetic alopecia, congenital hair shaft disorders, and telogen effluvium (TE) (Table 1).5,6
There are just a few descriptions of trichoscopic findings in patients with LAHS.5
In 2015, Rakowska et al. published a series comparing the dermoscopic findings of 89 children with LAHS, AA, TE, and healthy controls. The characteristic trichoscopy findings in LAHS were, solitary rectangular black granular structures, solitary yellow dots, and a predominance of follicular units with single hairs.5 In our series we found “dirty dots” (9/12), granular rectangular structures (5/12), and single yellow dots too (3/12); these findings were like those previously published by Rakowska et al. Herein we present new and not previously described findings (Table 2).
Clinical and trichoscopic findings in patients with LAHS.
| Patient | Gender | Age | Comorbidities | Motive of the visit | Vellus hair | Dirty dots | Scalp scales | Textile fibers | Cadaveric hairs | Blue and red dots | Granular rectangular structures | Loose fragments of hair shaft | Perifollicular hyperkeratosis | Pigmented network | Hair casts | Exclamation-mark hairs | Single yellow dots | Proximal coiled hair | Crusts on the scalp | Transverse bright bands | Flame hair | Dystrophic anagen hairs | Bended hairs |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 5 | Low stature | Hair loss | + | + | + | + | + | + | + | + | + | + | + | + | |||||||
| 2 | M | 4 | No | Hair loss | + | + | + | ||||||||||||||||
| 3 | F | 7 | No | Hair loss | + | + | + | + | + | + | + | + | + | + | + | + | |||||||
| 4** | F | 2 | No | Sparse hair | + | + | + | + | + | + | + | + | + | + | + | + | |||||||
| 5** | F | 6 | No | Sparse hair | + | + | + | + | + | + | |||||||||||||
| 6 | M | 1.5 | Bilateral congenital cataract | Sparse hair | + | + | |||||||||||||||||
| 7* | F | 8 | Uncombable hair | Hair does not grow | + | + | + | + | |||||||||||||||
| 8* | F | 6 | Uncombable hair | Hair does not grow | + | + | + | + | + | ||||||||||||||
| 9 | F | 3 | Infantile hemangioma | Hair does not grow | + | + | + | + | + | + | |||||||||||||
| 10 | M | 2 | No | Hair does not grow | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |||
| 11 | M | 6 | No | Hair does not grow | + | + | + | + | + | + | + | ||||||||||||
| 12 | F | 3 | No | Hair does not grow | + |
F: female; M: male.
Although signs such as dirty dots or single yellow dots can be present in diseases such as AA, trichoscopy added to anamnesis and physical examination can be an additional tool to diagnose LAHS at the office and help to reduce parental anxiety by explaining how favorable the prognosis of this condition really is.
Conflicts of interestNone declared.



