





A 30-year-old man with no relevant past medical history presented with a lesion on the lower helix of the right ear that had first appeared several months earlier. The lesion was asymptomatic and its growth had remained stable since it first appeared. The patient reported no history of trauma at the site and had no similar lesions at other sites.
Physical ExaminationPhysical examination revealed a soft, raised, well-defined, erythematous-violaceous tumor approximately 1cm in diameter that had a smooth surface and was not painful to the touch (Fig. 1).
Histopathology
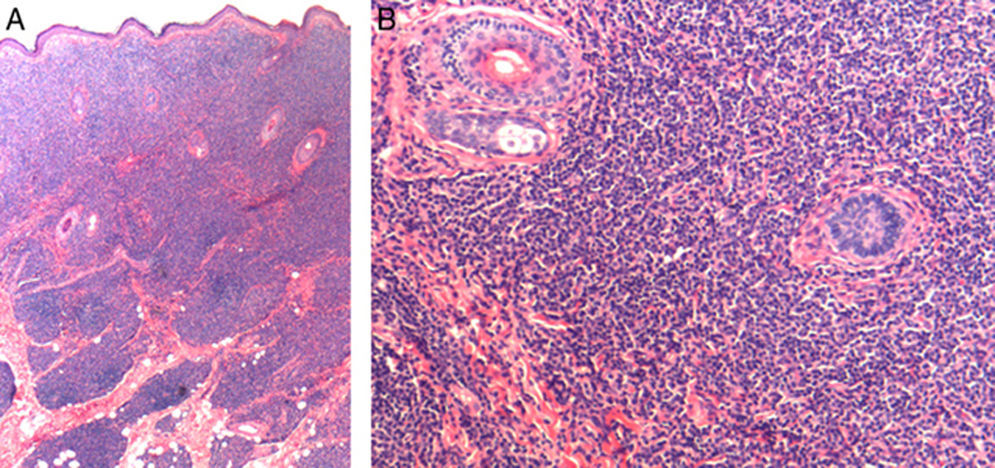
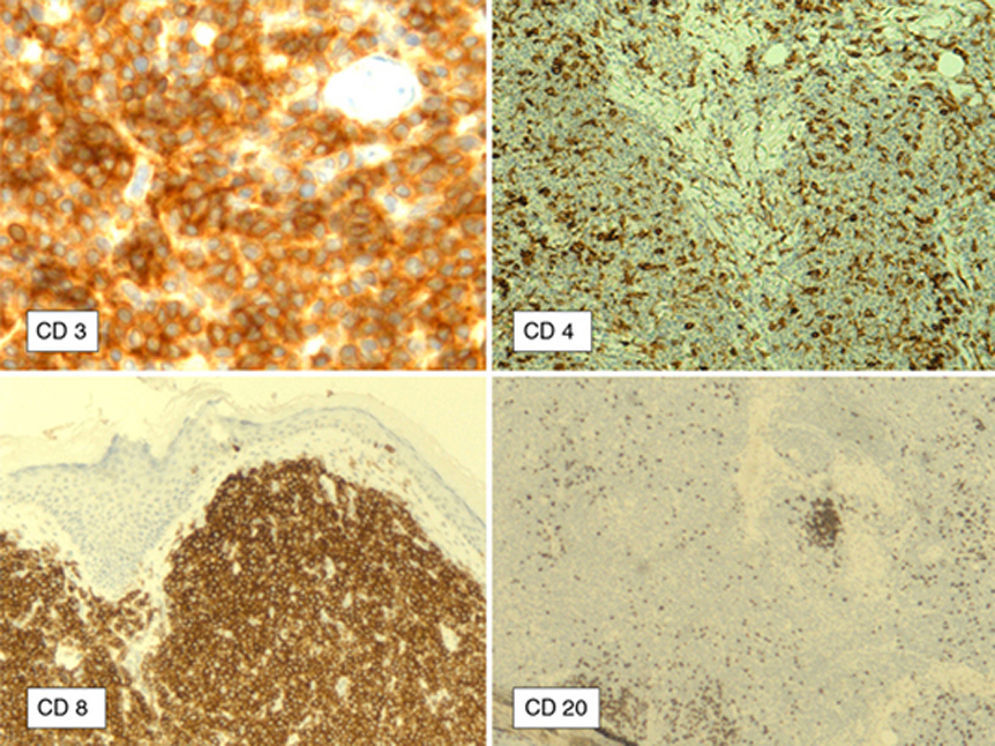
Hematoxylin-eosin staining (Figs. 2A and B) revealed a dermal lymphoid infiltrate composed of small to medium-sized lymphocytes with little atypia, no mitotic figures, and no phenomena of avascular necrosis or epidermotropism. In addition, a grenz zone separating the lesion from the dermis—which was completely spared—was also observed. Immunohistochemical staining was clearly positive for the CD3 and CD8 markers, partially positive for CD4, and negative for CD20 and CD30 (Fig. 3).
A blood workup revealed no alterations and a computed tomography study of the abdominal and pelvic region was entirely normal.
What Is Your Diagnosis?
DiagnosisIndolent CD8+ lymphoid proliferation of the ear.
Clinical Course and TreatmentComplete excision of the lesion was performed, followed by closure by plasty. No recurrence was detected during 2 years of follow-up.
CommentIndolent CD8+ lymphoid proliferation of the ear, first described by Petrella et al. in 2007, is a rare lymphoproliferative process that is not considered to be a cutaneous T-cell lymphoma according to the 2005 classification of the World Health Organization–European Organization for Research and Treatment of Cancer. Although it presents immunophenotypic characteristics also seen in aggressive CD8+ T-cell lymphomas, this new indolent lymphoproliferative process is probably a phenotypic variant of primary cutaneous CD4+ small-medium pleomorphic T-cell lymphoma, as first suggested by Beltraminelli et al. in 2009.1,2 Clinically, the entity is characterized by slow-growing lesions confined to a single cutaneous site, usually the ears or acral sites. In the cases reported to date, the entity has exhibited indolent clinical behavior and shown no signs of systemic involvement.1–3
Cutaneous CD8+ T-cell lymphomas were initially considered to be aggressive lymphomas with frequent extracutaneous involvement and poor prognosis. Subsequently, CD8+ lymphomas with a favorable prognosis—which did not match the original descriptions—were reported. In 2007, Petrella et al.3 reported for the first time 4 cases of a nonaggressive, nonepidermotropic, monoclonal, CD8+ lymphoid proliferation on the ear that did not appear to belong to any of the recognized types of cutaneous T-cell lymphoma. Other cases with the same clinical, histologic, and immunophenotypic characteristics were subsequently reported, prompting various authors to suggest that this new entity might be a new phenotypic variant of primary cutaneous CD4+ small-medium pleomorphic T-cell lymphoma.1,2,4–6
Physical examination of these indolent cases usually reveals an asymptomatic, slow-growing, erythematous nodule on the helix of the ear measuring approximately 1cm in diameter.1,2 Clinical differential diagnosis of this entity includes conditions such as cutaneous pseudolymphoma (benign lymphocytoma cutis) caused by Borrelia burgdorferi infection or by ear piercing. Histopathologic differential diagnosis includes benign lymphocytoma cutis, reactions to insect bites, discoid lupus erythematosus, panniculitis-like subcutaneous lymphoma, polymorphous light eruption, and angiolymphoid hyperplasia with eosinophilia, and less frequently primary cutaneous B-cell lymphoma. The CD8+/CD4- immunophenotype can be seen in CD8+ mycosis fungoides, pagetoid reticulosis, aggressive CD8+ primary lymphoma, prolymphocytic variants of leukemia, CD8+ lymphomatoid papulosis, and other conditions.1
Histologically, the entity is characterized by a dense dermal infiltrate of CD8+ T cells with a lymphoblast-like appearance, T-cell clonality, and no epidermotropism. The lymphoid infiltrate is composed of medium-sized pleomorphic cells with irregular nuclei and scant cytoplasm. There is no evidence of necrosis, mitosis, ulceration, or angiodestruction.6 Immunohistochemical staining is consistently positive for the CD3 and CD8 markers, while there is little expression of CD20, CD4, CD30, and CD56.4–6
Although in some cases the histopathologic appearance suggests a high-grade lymphoma, the clinical behavior of the entity is benign and therefore it is essential to differentiate it from other cutaneous CD8+ lymphomas that are associated with a poorer prognosis in order to avoid aggressive and unnecessary treatments.2,3
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Heras-González S, Aspe-Unanue L, González-Pérez R. Nódulo en el pabellón auricular. Actas Dermosifiliogr. 2017;108:581–582.


