


Lichen nitidus is an uncommon inflammatory dermatosis whose etiology is not well understood. It was first described by Pinkus in 1901 and its typical clinical and histopathological presentation are diagnostic in the majority of cases.1 The term Wolf isotopic response was coined in 1995 to refer to the appearance of a dermatosis on areas of skin with previous lesions that had healed and that bore no relationship with the new lesions.2 A recent classification defined the isotopic coresponse as the presentation of a dermatosis that develops in the same area of skin as another previously present but still active dermatosis.3
We present the case of a 38-year-old man with a past history of ulcerative pancolitis, recurrent episodes of acute pericarditis, and Graves disease. Important findings in his dermatologic history were universal alopecia areata treated with 5% minoxidil, topical and systemic steroids, and 0.001% diphencyprone to the scalp, and vitiligo that affected the head, trunk, penis, and limbs, treated with narrowband UV-B with a cumulative dose of 78.10J/cm2. After phototherapy, follicular repigmentation was observed in some macules on his scalp and back.
Eighteen months later, the patient was seen in dermatology for a 2-month history of multiple erythematous papules of 1 to 2mm in diameter, present exclusively on the achromic macules on his legs (Fig. 1), and nail dystrophy in the form of trachyonychia with longitudinal ridges on the nails of the hands and feet (Fig. 2).


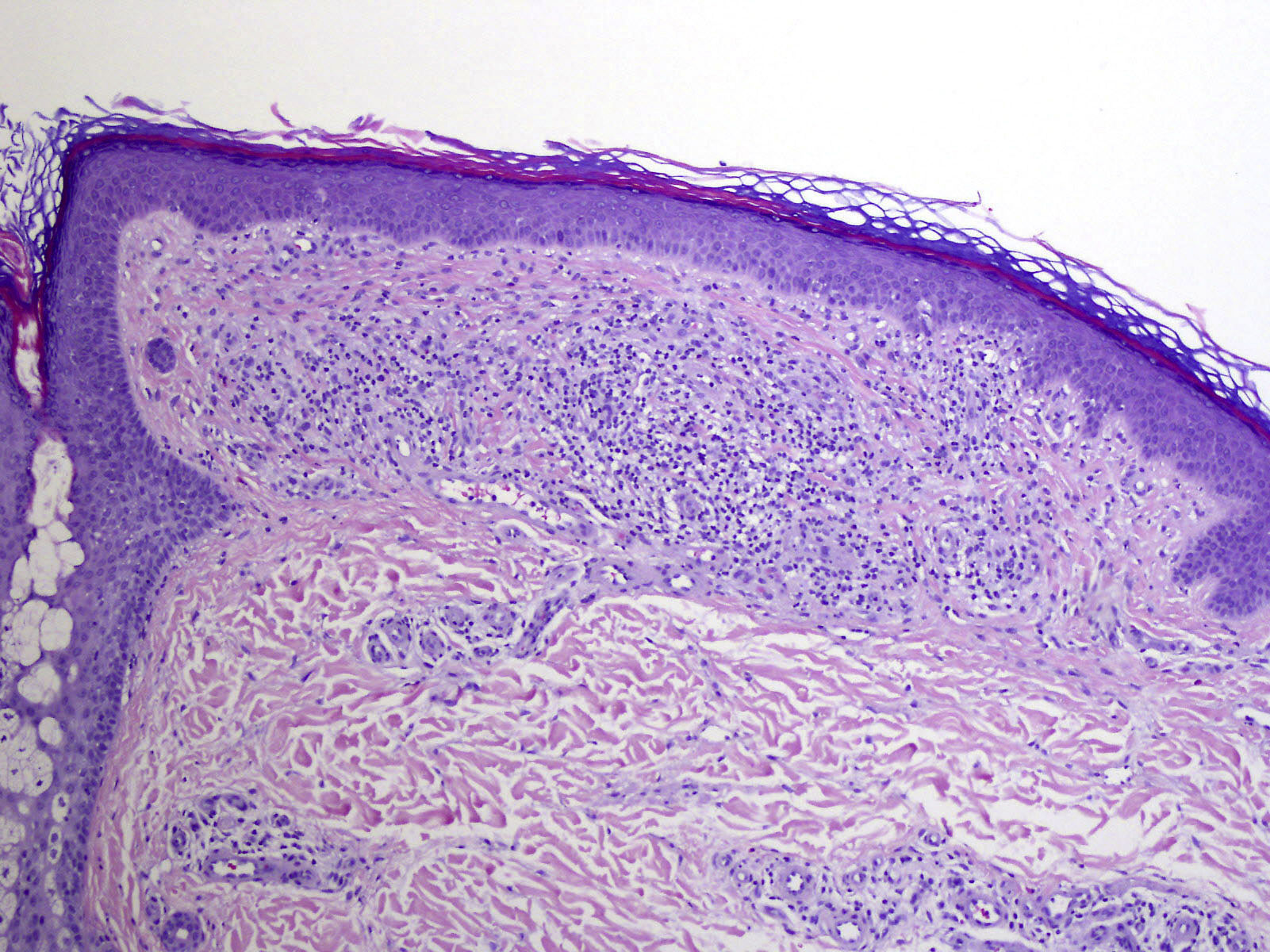
Histology of the skin lesions revealed a lymphohistiocytic infiltrate in the papillary dermis limited laterally by downward extensions of the epidermis, forming the pattern typical of lichen nitidus. There was mild epidermal atrophy and parakeratosis at the center of the papule (Fig. 3).
The skin lesions regressed almost completely after treatment with 0.1% mometasone. No improvement was observed in the nail lesions after treatment with nail lacquer containing 8% clobetasol, or subsequently with topical 0.1% tacrolimus.
During follow-up of the patient's dermatologic condition, he was diagnosed with Sjögren syndrome, thymic hyperplasia, and dysautonomy presenting clinically as episodes of severe hypotension. At the time of writing, the patient was being investigated for a possible autoimmune autonomic gangliopathy and was on treatment with intravenous immunoglobulin, pending precise definition of his autoimmune disease.
The appearance of skin lesions at the same site as a distinct previous dermatosis, with no relationship between the 2 conditions, has classically been described as the Wolf isotopic response.2 In the literature, the primary dermatosis in most cases has been metameric herpes zoster or lesions due to herpes simplex.4 It is thought that this predominance of herpetic lesions has been overestimated as a result of a memory bias on the part of the patient, as herpes zoster or simplex lesions are easily remembered. But other dermatoses distinct from herpes zoster or simplex lesions have also been reported, including cutaneous leishmaniasis, erythema multiforme minor, pityriasis rosea, and other noninfectious dermatoses.4,5
A new classification of these dermatologic phenomena has recently been proposed. This classification describes the isotopic coresponse phenomenon, which refers to the appearance of skin diseases at the same anatomic site as other previous dermatoses but, in contrast to the classic Wolf isotopic response, the previous dermatosis is still active at the time of appearance of the second skin disease,3 as in our patient. We have found 4 reports in the literature that correspond to the isotopic coresponse phenomenon. In all 4 cases the diseases were vitiligo associated with lichen planus.3
The etiology and pathogenesis of the Wolf phenomenon isotopic are still unknown, though some studies suggest an alteration of immunity limited to the area of the lesions. Inadequate regulation of the immune system has 2 clinical presentations. Activation of the immune system provokes the appearance of granulomatous and lichenoid lesions, whereas the inhibition of the system will facilitate infections or the formation of neoplastic lesions.6
We draw attention to the peculiarities of our case, in which the primary dermatosis was not of infectious origin and the premise that the secondary dermatosis appears over areas of skin in which the previous lesions had resolved was not satisfied, meaning that, according to the new classification, this was not a Wolf isotopic response but rather an isotopic coresponse phenomenon.3
The nail lesions were not biopsied, and we cannot therefore state whether these lesions were of lichenoid origin7 or were lesions related to the patient's alopecia areata,8 a more common association according to the literature.
The association between lichen nitidus and other systemic immunologic alterations should also be remembered,9 such as the patient's previously described complex autoimmune condition and the very rare nature of this variant of the isotopic coresponse phenomenon not previously described in the literature.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Oscoz-Jaime S, Loidi-Pascual L, Tuñón-Álvarez MT, Yanguas-Bayona JI. Liquen nitidus sobre vitíligo: nueva variante del fenómeno de co-respuesta isotópica. Actas Dermosifiliogr. 2016;107:860–861.


