





Aesthetic dermatology offers many minimally invasive therapies that can help our patients age gracefully and discreetly. Because it is hard to systematize these treatments to make patients aware of the options they have for the area of the face they want to improve, at Clínica Dermatológica Internacional, we have developed the Skin Age Management (SAM) protocol. In this article, we describe this protocol designed to help doctors and patients to better understand and plan available treatments, underlining the advisability of combining techniques with the goal of achieving discreet changes to obtain what we consider to be optimum results, based on our experience at our center.
La dermatología estética hoy en día contempla múltiples tratamientos mínimamente invasivos que pueden ayudar a envejecer a nuestros pacientes con elegancia y discreción. Dado que puede resultar difícil sistematizarlos para que el paciente sea consciente de las posibilidades que tiene en función del área que quiere mejorar, desde Clínica Dermatológica Internacional hemos elaborado el protocolo Skin Age Management (SAM). En este artículo describimos este protocolo —dirigido a ayudar a médicos y pacientes a conocer mejor y planificar los tratamientos disponibles, que refuerza el mensaje de la idoneidad de la combinación de técnicas con la filosofía de lograr cambios discretos para obtener los resultados que consideramos óptimos—, basado en la experiencia de nuestro centro.
Modern aesthetic dermatology offers a broad range of minimally invasive treatments that can help our patients to age elegantly and with discretion. It can be difficult to present our patients a systematic overview of these treatments so as to ensure that they are aware of all of the options available to them in the areas they want to enhance. At Clínica Dermatológica Internacional we have developed a structured protocol to address this need. The aim is to help physicians and their patients to better understand the options and to decide on a treatment plan. It also reinforces the message that the ideal approach can often be found in a combination of different techniques1,2 and reflects our philosophy that the results we consider optimum are obtained by implementing a series of discreet changes. Our name for this this protocol is SAM—an acronym for Skin Age Management. When patients come to our dermatology office to consult us on how they can improve their appearance, we show them the SAM diagram, which summarizes the options available and allows us to organize our recommendations and plan the treatments (Fig. 1).
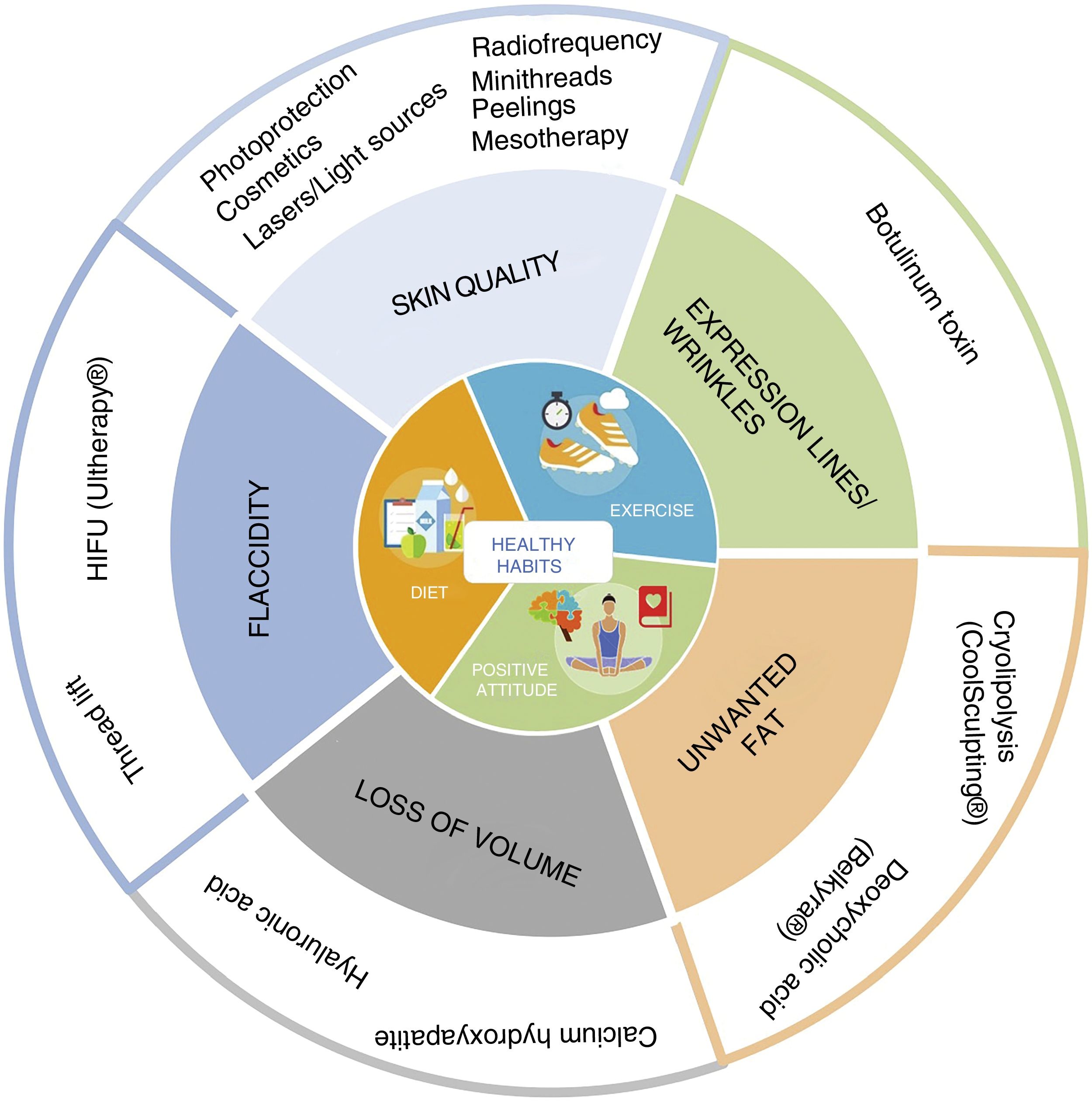
Diagram of the Skin Age Management (SAM) Protocol. At the center of the wheel are recommendations for a healthy lifestyle, a vital component of any treatment intended to achieve elegant and discreet aging. The outer ring shows the different treatments available for each indication. Any approach to facial aging should start with skin quality, then address expression lines, and continue, if necessary, with the other treatment options indicated. HIFU indicates high-intensity focused ultrasound.
In the central panel, we underscore the fact that the most important factor in aging with elegance and discretion is to maintain a positive mental attitude3 and a healthy lifestyle, including a varied and balanced diet (a skin healthy diet4), not smoking, and engaging in moderate physical exercise every day.5
In this article, we will describe the various options available, depending on the areas the patient wishes to improve. Although most of these technique can be used on people from any geographical area, this article is based on our daily experience treating patients who mostly have Fitzpatrick I to IV phototypes.
Skin QualityThe best approach to improving skin quality involves an assessment by a dermatologist, who establishes a cosmetic protocol and identifies the problems that can be modified or treated:
The first step is never to forget that sunscreen is the best cosmetic. The daily use of a sunblock to protect the skin will prevent photoaging as well as having other beneficial effects.6 In addition to the regular use of sunscreen, we also often recommend cosmeceutical products that contain molecules with proven antiaging properties.
Retinoic acid is the most effective of these ingredients and we generally recommend its application 2 or 3 nonconsecutive nights a week, adjusting the regimen in patients with sensitive skin or when there are specific environmental factors. Other ingredients that have shown some efficacy include vitamin C, alpha hydroxy acids (such as glycolic acid), and other vitamin A derivatives, such as retinol, etc.7
The current trend is to offer each patient an individualized cosmetic protocol including personalized cosmetics adapted to the characteristics of their skin.
If the patient has solar lentigines or other signs of photoaging, we recommend alexandrite or Q-switched laser therapy.8 In the case of telangiectasias and erythema we use vascular lasers, including 595-nm pulsed dye laser,9 1064-nm neodymium:yttrium-aluminum-garnet laser,10,11 and medical intense pulsed light.12 To treat severe photodamage, particularly in patients with poikiloderma, we used a combination of several light sources: intense pulsed light, stain removal lasers, as well as vascular and nonablative fractional lasers, such as 1550-nm erbium:glass and 1927-nm thulium.13
In patients with melasma, we have observed better responses to treatment in our clinic with low energy lasers (such as 1927-nm thulium)14 or gentle exfoliating procedures15 in combination with the application at the patient's home of depigmenting formulas containing retinoic acid and hydroquinone.16
For the treatment of irregularities in the form of lines and wrinkles (in particular the vertical barcode lines on the upper lip and crow's feet around the eyes),17 scars (like those caused by acne or surgical procedures),18,19 and open pores,20 we recommend using fractional ablative technologies, such as carbon dioxide lasers. These have been shown to be better than classic lasers in terms of patient tolerance and the occurrence of adverse effects.21,22
To enhance skin luminosity, we mainly use mesotherapy with hyaluronic acid (multiple microinjections of this substance into the area of the face, neckline, or back of the hands to be treated)23,24 and platelet-rich plasma (PRP). PRP involves drawing blood from the patient, separating the growth factors contained in the platelets by centrifugation, activating the platelet membranes, and intradermal injection of the resulting PRP in the form of mesotherapy).25–27 Radiofrequency devices have also been used for many years to make skin more luminous; they also have a slight firming effect.28,29
If facial skin has atrophied or thinned, PDO mini threads can be implanted by injection into the deep dermis to induce neocollagenesis.30
Expression LinesBotulinum toxin is the technique that has revolutionized nonsurgical rejuvenation methods. It is a safe and effective technique that provides natural results when used carefully. The use of botulinum toxin alone without other treatments is not an ideal approach because it only improve wrinkles; in most patients the best results are obtained when it is used in combination with other techniques to obtain more harmonious results.31Table 1 lists the 10 commandments for optimum use of botulinum toxin in facial rejuvenation.
The Ten Commandments of Botulinum Toxin63
| 1. Botulinum toxin or “botox” reduces expression lines. It is an ideal treatment for controlling expression lines, such as the glabellar lines between the brows, periocular crow's feet, and frown lines on the forehead. The aim is to relax the expression in order to conceal accumulated tension. Loss of volume, poor skin quality and laxity should be treated using other dermatological techniques. |
| 2. Botulinum toxin is safe. In over 50% of cases it is used for medical purposes, such as the treatment of migraine headaches, excessive sweating, nervous tics, strabismus, etc. Due to its excellent safety profile, the treatment is often used in children to treat abnormal muscle movements. |
| 3. Be careful with the dose. Appropriate doses must be used to achieve natural results and preserve the patient's facial expressivity. The muscles should be relaxed rather than paralyzed with excessively high doses. Conversely, excessively low doses can lead to an overly short durations of effect. |
| 4. Botulinum toxin prevents the formation of wrinkles. It has a preventive effect on aging because it “educates” the facial muscles. |
| 5. Every patient is different. Not all patients require the same injection technique. Since the anatomy of every patient's face is different, the injection sites and the dose used must be adjusted in each case to achieve natural results. The injection technique for men and women is totally different. For example, the gull wing shape of the eyebrow in women is totally different from the shape of the male eyebrow, which tends to be straighter and situated closer to the eyelid. |
| 6. Treatment with botulinum toxin must be repeated. We recommend repeating treatment every 4 to 6 months. Repeat treatment should take place before the effect of the previous administration disappears. |
| 7. The approach must be global. The only way to achieve natural results is by treating the face as a whole. Consequently, the entire face should be treated to relax all the “depressor” muscles that configure facial expression. |
| 8. Botulinum toxin treatment can make us feel better. When properly injected the treatment reduces the appearance of worry and sadness. It has been shown that this effect on our facial expression also improves our mood. We feel happier because we look happier. |
| 9. Bad results are due to bad technique. Botulinum toxin is like a scalpel: the results can be good or bad depending on the technique. Grotesque outcomes are the result of misuse. |
| 10. Less is more. The most elegant results are achieved through discreet changes. If someone asks you “What have you done?”, change your doctor. The goal is for everyone to notice that you look better without realizing that you have had treatment. |
Several non-invasive procedures used to treat body fat can also be used to treat a double chin by reducing submental fat. The appearance of a double chin is an age-related change that worries a large number of patients and is sometimes neglected by aesthetic dermatologists. Treating submental fullness produces a strong emotional impact and improves the patient's self-image.32 In a study of 600 men recently published by an American team, the double chin was the third most likely motive for treatment cited by the respondents.33 In our experience, it could be the leading reason for consultation among men and a very common motive among women if the possibility of nonsurgical treatment were more generally known. Until relatively recently, surgical liposuction was the only effective way to eliminate submental fat. Today, there are 2 other safe and effective methods for eliminating submental fat: cryolipolysis with the Coolsculpting® device and injection with deoxycholic acid (marketed in Europe for this indication as Belkyra®.
Submental Fat Elimination With CryolipolysisSelective cryolysis of subcutaneous fat (or cryolipolysis) involves the application on an area of the skin of a device that pulls the skin in by suction and cools it to induce inflammation (initially leading to lobular panniculitis) and the specific destruction of adipocytes. Given the greater sensitivity to cold of fat cells, the treatment does not damage the epidermis or other structures.34 For the treatment of localized fat, the Coolsculpting® device is the technology that has been most validated. It was the first cryolipolysis system to be developed and approved by the regulatory agencies and its effectiveness has been demonstrated. Although other treatments, such as other cryolipolysis systems and devices based on radiofrequencies or focused ultrasound, can be considered, Coolsculpting® is the only device that has been shown to be safe and effective for this indication; it achieves predictable results and a high degree of patient satisfaction. Coolsculpting® is a simple technique: no anesthesia is required and there is no downtime after treatment. The Coolsculpting® device can also be used to treat other areas of the body, including the abdomen, flanks, back, as well as the inner aspect of the thighs and arms. Many authors have reported on the use of Coolsculpting® to eliminate submental fat. The mean reduction achieved was 2 mm of subcutaneous fat per session, as measured by ultrasound,35 or 33% of the fatty fold, as measured by a pleximeter after 2 sessions.36 A new method requiring shorter sessions of about 35 minutes in duration has been developed based on a redesigned applicator.37 In our experience, an approximate improvement of 20% can be observed in 1 session. Ideal candidates for this technique are patients whose weight is within the normal range and who have modestly pronounced fat deposits that are difficult to eliminate through diet or exercise. There is no limit to the number of sessions a patient can undergo, but in general we recommend 2 sessions separated by an interval of at least 1 month.
Deoxycholic Acid InjectionsThe other nonsurgical technique that should be considered when treating submental fat is deoxycholic acid.38 This is available in 2-mL vials of a 10-mg/mL solution (marketed as Belkyra® in Spain and Kybella® in the United States). The product was launched in Spain in 2017 and 2 years earlier in the United States.38 Before administration, the injection sites (1cm apart) are marked on the area to be treated using a template. Then the treatment is administered in subcutaneous injections of 0.2mL up to a maximum infiltration volume of 15 mL per session. The injections can be somewhat painful, making it advisable to use local anesthesia, cold, and analgesia. After infiltration, pain, swelling and bruising in the treated area is not uncommon. The most feared complication of this technique (rare when the injection sites are properly marked) is the accidental injection of the product into the marginal mandibular branch of the facial nerve, causing paralysis on 1 side of the mouth lasting for some months. Patients can undergo a maximum of 6 separate sessions separated by intervals of at least 1 month.39 The usefulness of this technique has been demonstrated in men, in whom it is recommended that a larger surface area be treated at the first session to obtain the best outcome.40
Volume LossIn the 1980s, the rise of cosmetic surgery led to a growing trend in surgical facelifts, a technique that was very effective in reducing visible wrinkles but tended to produce unnatural results. The use of dermal fillers first started to become generalized at the end of the 1990s. This was the first technique to address the problem of creating facial volume to compensate for the loss of volume secondary to changes in facial fat and bones.41 While some aesthetic protocols continue to include permanent fillers such as silicone,42 the most widely used fillers today are non-permanent products based on hyaluronic acid, calcium hydroxyapatite, and polylactic acid. The results obtained are constantly improving as a result our of greater understanding and knowledge of age-related anatomical changes and the way the products available should be applied.43
To properly apply a dermal filler, the first thing we must address is the diagnosis of the area to be treated. Over time, some of the facial convexities characteristic of childhood are lost, giving rise to areas of shadow around the eyes and mouth, which can give rise to an appearance of tiredness. The best way to correct these changes is with the prudent use of fillers. Another aspect that should be taken into account in any rejuvenation protocol is the so-called “triangle of youth”: the face of a young person is shaped like a triangle with the base across the forehead and the apex pointing downwards. With age, the triangle is inverted and the base moves to the lower part of the face: the face becomes wider and less oval. Consequently, adding volume to the lower third of the face should be avoided. Hyaluronic acid is our dermal filler of choice. It has the added advantage that an “antidote” exists in hyaluronidase, although the effect of the antidote may vary depending on the hyaluronic acid filler used.44 In Spain, hyaluronidase can only be obtained as a customized compound for off-label use; our protocol for its use can be found in Table 2. The other dermal filler we use is calcium hydroxyapatite, although the effect in this case is more collagen-inducing than filling. Currently we do not use any other fillers in our practice.
Protocol for Hyaluronidase Treatment.
| • A 300 UI vial of lyophilized hyaluronidase should be ordered from a compounding pharmacy . |
| • When required, the 300 UI vial should be diluted in 2 mL of physiological saline (such that every 0.1 mL contains 15 UI). |
| • Injection must be done slowly using a 32-gauge needle, with volumes of 0.05 to 0.1 mL per injection site (a dose of 7.5-15 UI). |
| • A pre-treatment test on the patient's forearm is recommended (although some authors argue that the test is the use of minimal doses), because of the possibility that some patients may be allergic or have an anaphylactic reaction. |
| • It is generally recommended that patients should be seen a week after administration to assess the need to repeat the treatment. |
In our opinion, the replacement of facial volume is secondary compared to other goals, such as improved skin quality, in the aesthetic patient. Even when the fillers used are temporary in nature, they should be used with caution because it has been observed that, in the long-term, excessive treatment or “filler fatigue” can give rise to an inharmonious appearance. Filler fatigue is caused by a decrease in skin elasticity, fibrosis, and the creation of an unnaturally wide face. All of these changes can occur not only because of excessive use of collagen-inducing fillers such as calcium hydroxyapatite (which induces fibrosis and may persist in the treated area for years45) but also owing to overuse of hyaluronic acid (which triggers an increase in profibrotic growth factors and collagen fibers types I and III).46 It has also been observed that fillers that have a greater degree of cross-linkage and the use of techniques such as superperiosteal injections can lead to more long-term effects47 and increase the likelihood of adverse events.48,49 Fillers are, therefore, a useful tool provide they are used in moderation and applied by someone who has a great deal of knowledge about facial anatomy and in combination with other, complementary, techniques.
FlaccidityThe 2 nonsurgical techniques we currently use to treat skin flaccidity without increasing volume are ultrasound (using either high-intensity focused ultrasound [HIFU] or microfocused ultrasound) and thread lifting.
UltrasoundThere are several devices on the market designed to reduce skin laxity.50 While non-ablative techniques based on external radiofrequency may have some tightening effect,51 in our clinical experience the actual clinical effect is minimal. In recent years, therefore, we have opted to use HIFU devices, which apply focused ultrasound waves at various depths. A device with the broadest range can focus the power at 1.5, 3, and 4.5 mm, modulating the frequency to 10, 7 and 4.5 MHz). This device can produce small thermal coagulation points in fat and fibromuscular tissue that have a tightening effect; tolerance is good and the procedure has very few side effects (infrequent bruising, tingling, or temporary muscle weakness), which resolve within a few days or weeks.52 While rare, more serious adverse effects may occur53; these could be related to poor technique or inappropriate use, underscoring the importance of proper training in the technique and an extensive knowledge of facial anatomy. This technique is ideal for patients with mild to moderate laxity or sagging along the jawline, on the neck, and around the eyes. It is particularly appropriate for correcting infraorbital laxity and for closing up the infrapalpebral space, where the edema that gives rise to “bags” accumulates).54 It achieves unobtrusive results within a month of treatment. The results are cumulative and can have a preventive effect, which is why some plastic surgeons have called HIFU a “facelift by installments”. For best results the procedure can be repeated every 6 to 12 months. HIFU can be combined with other noninvasive treatments.55,56
Thread LiftThread lifting is an interesting resource in any global approach to facial rejuvenation. The threads are easy to apply and do not add volume (making them ideal for use in the lower third of the face). Their tightening and firming effect can be used to reposition loose or sagging tissue.57 There are many types of lifting threads on the market (monothreads, barbed threads, cone threads, etc.). They can be grouped into 2 basic types.
On the one hand, we have simple, monofilament strands of polydioxanone (PDO) (monothreads), which are used to increase skin density. These threads are inserted with a needle into the deep dermis, where they trigger the formation of collagen and produce a revitalizing effect that can last between 3 and 9 months. The areas most often treated are the jawline, cheeks (to reduce the nasolabial folds), neck, and the neckline or décolletage. Other areas that can be treated using this technique include the eyebrows, arms, legs, and buttocks.30
On the other hand, we have PDO or poly-L-lactic acid (PLLA) threads with barbs, cones, and other kinds of hooks. These have a greater tightening effect because they facilitate anchoring, traction, and repositioning of the tissue as well as having collagen inducing properties. These threads are inserted into the hypodermis. They produce visible effects that last up to 1 year. The areas most often treated include the jawline and neck, although they can also be used to treat the cheeks and eyebrows.30,58 A mild and transient side effect of the insertion of both types of threads is bruising and edema at injection sites.
Final ReflectionsThe Art of the Aesthetic ConsultationThe doctor-patient relationship established in the initial consultation is the key to the clinician's empathy or “connection” with the patient. In Table 3, we list a series of suggestions we consider should be taken into account by any physician treating aesthetic patients with a view to attaining the optimum results for each patient. Following this advice can have a remarkably positive effect on patient satisfaction and loyalty as well as on adherence to the treatment. If we, as doctors, give greater importance to the art of the aesthetic consultation, we will feel more comfortable with ourselves and provide a reason why we can never be replaced by machines or robots.
Suggestions for Improving the Art of the Aesthetic Consultation.
| 1. Prepare for the consultation before seeing the patient. Ensure that the patient knows that you are waiting for them, that you are aware of the reason for their visit, and that they have your full attention. You only have one opportunity to create a good first impression, Dońt waste it. |
| 2. Focus all your attention on the consultation. The patient must feel that they are the center of your attention. Avoid interruptions from cell phones, conversations with staff or colleagues about other topics or other patients and make sure that no one comes in and out of your office. |
| 3. Be aware of your body language: do not sit too far away from the patient, look directly into his or her eyes. |
| 4. Obtain a complete medical history to rule out diseases or drugs that might influence the results of aesthetic treatments |
| 5. Ask the patient what cosmetic treatments (surgical or nonsurgical) they have undergone previously. |
| 6. Take pictures of a range of positions and different expressions. After undergoing a procedure, patients look much more closely at their faces and may, in some cases, blame the treatment for a pre-existing flaw or lack of symmetry. |
| 7. Be genuine. A patient will always know whether you really care or not. |
| 8. Use the power of touch. It is important to explore the patient's face sensitively with your hands so that they will feel that the evaluation has been complete. |
| 9. Give the patient a mirror and ask them to indicate what areas they would like to improve. |
| 10. Carefully assess the patient's expectations to ascertain whether they are realistic. If a patient has unrealistic expectations, be honest with them and do not recommend any treatment. The formula is as follows: satisfied patient = good aesthetic results –prior expectations. A patient who has unrealistically high expectations will never be satisfied. One sign that should ring alarm bells is a patient who complains about all the doctors who have previously treated them. |
In the field of dermatology and aesthetic medicine, we believe that there has been an absence of major innovations in recent years. In other words, there has been no revolution comparable to those that have transformed other areas, such as on-line shopping, urban mobility, the consumption of audiovisual content, information search, and interpersonal communication. In the field of aesthetics:
- -
Retinoic acid, which is still the most effective anti-aging ingredient in creams, has been on the market for over 40 years.
- -
Research on the effects of nutricosmetics59 has not, as yet, provided evidence of extraordinary benefits that would justify their routine use.
- -
Technology has not yet led to any disruptive innovations. The laser devices we use today for vein treatment, hair removal, photorejuvenation, and spot removal are similar, despite progressive optimization, to those we were using 15 years ago. While the new radiofrequency devices, intense pulsed light, and focused ultrasound have not offered exponential advances, we believe that cryolipolysis and the use of microwaves for the treatment of hyperhidrosis represent qualitative leaps in the technology in recent years.
Having had occasion to try most of the technologies currently used, many dermatologists involved in the treatment of aesthetic patients have come to the conclusion that the last truly disruptive innovation in this field was introduced over 15 years old: the liquid facelift, that is, the use of a combination of injectables (essentially botulinum toxin, dermal fillers, collagen inducers, and lifting threads) in a prudent and intelligent way. The term liquid facelift was coined by Mauricio de Maio, a Brazilian plastic surgeon who has been one of the promoters of the use of a combination of injectables to relax expression lines, compensate for loss of volume, and induce collagen productio.60
In our clinic, we classify liquid lifting techniques into 5 types depending on the complexity of the technique (from lower to higher complexity) (Fig. 2). In patients who can benefit from this approach, after a meticulous physical examination and after assessing and discussing the patients expectations, we decide on what level of liquid facelift is appropriate and will achieve the most natural results and satisfy the patient.
The Importance of the Emotional Domain
Generally, when patients are informed about what can be achieved with rejuvenation techniques, the information they are given is usually framed in terms of objective outcomes (the reduced visibility of the wrinkle, the removal of a mark or discoloration, and so on). It is vital, however, for the clinician not only to clinically assess the individual patient but also to gain a better understanding of their emotions, values and expectations in order to achieve the highest possible degree of satisfaction. The patient will understand the message better if rather than saying that the procedure will improve a wrinkle, the physician explains that the aim of the technique is to eliminate a facial expression associated with annoyance, fatigue, or sadness.
Using these minimally invasive techniques, dermatologists can achieve an improvement in the patient's mood and quality of life.61 Messages like those exemplified in the previous paragraph reinforce the positive feedback loop between the result obtained, what the patient perceives, and what was discussed in the initial consultation. For example, it has been reported that patients who cannot look sad may experience an improvement in mood.62
ConclusionsTo conclude, let us reflect on the messages that summarize the global approach we propose to patients who consult us for aesthetic procedures:
- 1)
Skin quality is the first thing that should be improved. Removal of pigmented stains and spots, vascular lesions, and scars as well as brightening the skin is a priority in any facial rejuvenation protocol.
- 2)
The best results can be achieved by using a combination of different treatments.
- 3)
We recommend using only low doses of botulinum toxin on the face.
- 4)
Excessive use of fillers should be avoided as it can lead to an unnatural appearance in the medium and long term.
- 5)
Techniques that tighten the skin are recommended for the lower third of the face. Techniques designed to add volume should be minimized in this area because the aging process leads to an accumulation of tissue in this region.
- 6)
Reducing submental fat should be considered in facial rejuvenation. This can be achieved using effective and minimally invasive techniques, such as cryolipolysis and injection lipolysis with deoxycholic acid.
- 7)
Every patient who visits an aesthetic dermatologist should be made aware that less is more and that the most natural results are achieved by making a series of discreet changes.
- 8)
Since aging is an ongoing process, antiaging techniques also have to be repeated regularly to ensure a continuous process.
- 9)
We treat people and not areas of the body. The key to our practice is an empathetic approach based on the patient's psychological and emotional health.
The authors have a private practice and regularly use the technologies and products described. However, the authors have no commercial or advertising links with the suppliers of any of these products.
Please cite this article as: Ruiz-Rodriguez R, Martin-Gorgojo A. Abordaje facial global del paciente estético: protocolo Skin Age Management. Actas Dermosifiliogr. 2019;110:197–205.


