

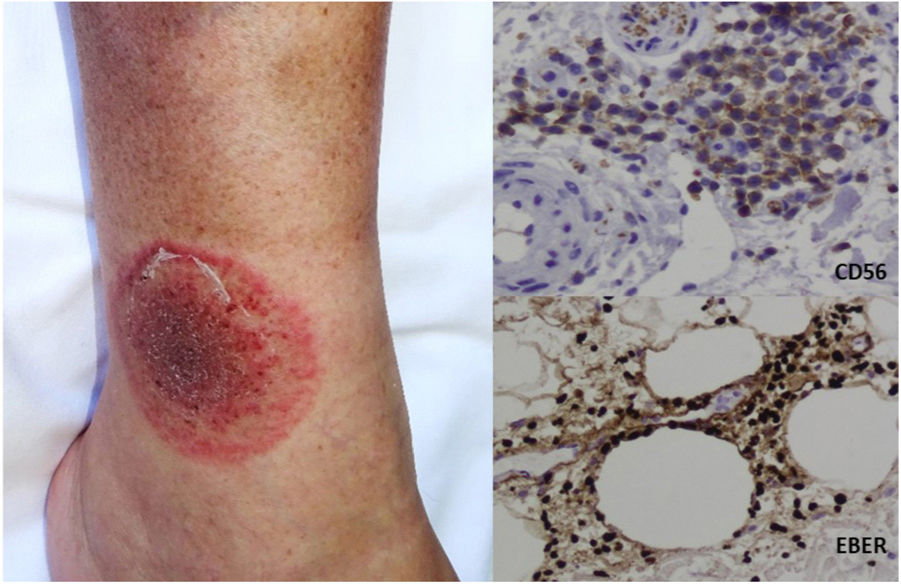
The patient in the image was a 62-year-old man who attended the dermatology clinic with a scaly oval plaque on the lower third of the right leg that had not responded to antifungal agents. Examination revealed an erythematous-violaceous plaque with a more active border and peripheral scaling. The scaling was assessed using potassium hydroxide testing and dermatophyte culture, both of which yielded negative results. Punch biopsy of the margin of the lesion was eventually performed. The histology workup revealed an atypical diffuse perivascular inflammatory lymphocytic infiltrate with immunohistochemistry markers that were positive for EBER and CD56. The patient was diagnosed with extranasal extranodal natural killer/T-cell lymphoma, nasal type (Fig. 1).
Extranodal natural killer/T-cell lymphoma, nasal type is a generally aggressive lymphoma found in the upper respiratory tract. The skin is the second most common location after the nasal cavity. The dermatologic lesions usually take the form of plaques or tumors, which are sometimes ulcerated.
The clinical heterogeneity of the lymphoproliferative processes may delay the diagnosis. This image reflects the importance of biopsying lesions that do not respond to empirically initiated treatment.



