
Immigration is a reality that cannot be ignored and that provides new professional challenges.1 As a result, the number of publications related to immigration has increased markedly.2–7
Among the skin conditions affected by immigration are sexually transmitted diseases, with some articles reporting a greater incidence of carriers of condyloma acuminata among immigrants.3–5
The aim of this study was to answer the question posed by the title of this article, though any conclusions are clearly limited to the population actually studied.
We retrospectively included male patients with a clinical and histologic diagnosis of condyloma acuminata who were seen in the dermatology clinic of our hospital between February 18, 2008 and December 31, 2011.
We undertook chart review of these patients, and noted the following information: autochthonous or immigrant (including country of origin in the latter case), age, site/number/duration of lesions, presence of human papillomavirus (HPV) in skin lesions (using CLART Clinical Arrays from GENOMICA), associated sexually transmitted diseases, risky sexual practices, treatments received, and outcome.
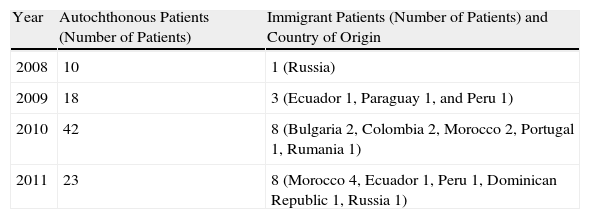
In total, the medical records from 113 patients were retrieved. Of these patients, 93 (82%) were autochthonous and the rest were immigrants who had been living in Spain for at least 6 months. The origin of these patients was extremely varied (Table 1).
Number and Country of Origin of Patients.
| Year | Autochthonous Patients (Number of Patients) | Immigrant Patients (Number of Patients) and Country of Origin |
| 2008 | 10 | 1 (Russia) |
| 2009 | 18 | 3 (Ecuador 1, Paraguay 1, and Peru 1) |
| 2010 | 42 | 8 (Bulgaria 2, Colombia 2, Morocco 2, Portugal 1, Rumania 1) |
| 2011 | 23 | 8 (Morocco 4, Ecuador 1, Peru 1, Dominican Republic 1, Russia 1) |
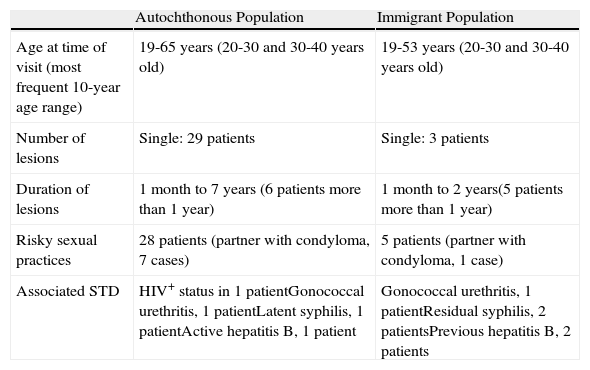
The remaining demographic information is presented in Table 2. There were no significant differences in terms of genital or perianal site of lesions. Two autochthonous patients had oral mucosal lesions.
Clinical and Epidemiological Characteristics.
| Autochthonous Population | Immigrant Population | |
| Age at time of visit (most frequent 10-year age range) | 19-65 years (20-30 and 30-40 years old) | 19-53 years (20-30 and 30-40 years old) |
| Number of lesions | Single: 29 patients | Single: 3 patients |
| Duration of lesions | 1 month to 7 years (6 patients more than 1 year) | 1 month to 2 years(5 patients more than 1 year) |
| Risky sexual practices | 28 patients (partner with condyloma, 7 cases) | 5 patients (partner with condyloma, 1 case) |
| Associated STD | HIV+ status in 1 patientGonococcal urethritis, 1 patientLatent syphilis, 1 patientActive hepatitis B, 1 patient | Gonococcal urethritis, 1 patientResidual syphilis, 2 patientsPrevious hepatitis B, 2 patients |
Abbreviations: HIV, human immunodeficiency virus; STD, sexually transmitted disease.
We did not find any differences between groups in terms of the presence of HPV as determined by the Clinical Arrays (GENOMICA) assay. The most frequent HPV serotypes were 6 and 11. An immigrant patient was positive for HPV 6 and an autochthonous patient was positive for HPV 61 and 81.
We found no differences in the type of treatment needed to control the lesions or whether monotherapy or combination therapy was administered. In both groups, the treatments used, from most frequent to least frequent, were cryotherapy, podophyllin, and topical imiquimod. Likewise, no differences were observed in terms of outcome for the 2 groups.
The analysis of articles related to an increase in sexually transmitted diseases in the immigrant population in Spain points to greater frequency of HPV infections among female immigrant prostitutes.3 However, this observation is not well established in male immigrants.4,6 Albares et al.,4,5 in studies in Spain, did not find any significant differences in patients with condyloma acuminata among immigrant and autochthonous populations, but they did not analyze men and women separately.
In our series, no differences were found between immigrant and autochthonous populations on comparing the characteristics of patients with condyloma acuminata, although immigrants tended to wait longer before seeking medical attention. This finding could be explained by a possible lack of awareness of the health system or cultural taboos concerning sexually transmitted diseases among male immigrants.
Please cite this article as: Díaz Díaz RM, Garrido Gutiérrez C, Navarro Cantero A, Ruíz Bravo-Burguillos E. Condilomas acuminados en varones. ¿Existen diferencias entre población inmigrante y autóctona? Actas Dermosifiliogr. 2014;105:519–520.


