






Certain skin conditions, such as vitiligo, acne, vascular malformations, and surgical scars, can impair the quality of life of pediatric patients, especially adolescents—even to the point of hindering psychosocial development.
We review the cases of 6 patients with discoloration or scarring, predominantly of the face, who attended our cosmetic camouflage workshops from January through December 2012. The quality-of-life impact of their skin disorder was assessed before and after workshop attendance.
Cosmetic camouflage is an easily replicated, cheap, and noninvasive adjunctive treatment of great potential value in managing skin conditions that impair the physical and emotional well-being of pediatric patients.
En la edad pediátrica existen determinados trastornos cutáneos que pueden afectar a la calidad de vida de los niños y en especial a los adolescentes, e incluso representar un obstáculo para su desarrollo psicosocial, como son el vitíligo, el acné, las malformaciones vasculares o las cicatrices posquirúrgicas.
Se revisaron un total de 6 pacientes con alteraciones pigmentarias y cicatriciales de predominio facial que participaron en el taller de camuflaje de nuestro servicio desde enero a diciembre de 2012, con evaluación del impacto de su trastorno cutáneo en la calidad de vida antes y después de la sesión de maquillaje terapéutico.
El maquillaje corrector es una técnica complementaria, fácilmente reproducible, económica y no invasiva que puede ser de gran utilidad en el manejo de enfermedades dermatológicas con repercusión en la esfera física y emocional de pacientes en la edad pediátrica.
The psychosocial development of pediatric patients can be significantly hindered by certain types of skin conditions,1 such as pigmentary disorders (particularly vitiligo), vascular abnormalities, inflammmatory conditions including acne,2,3 rosacea, and surgical scars or burn scars.
Pediatric patients experience greater quality-of-life impairment if there is facial involvement, particularly with vitiligo.4,5 The impact on physical appearance is greater for patients with darker skin phototypes. After 10 years of age, children develop stronger social relationships and become more aware of their appearance, so skin disorders can get in the way of their social development.6
Camouflage therapy using corrective cosmetics is a useful adjunct to other management measures, as it helps limit the impact on quality of life.7,8
We reviewed the pediatric patients with discoloration or scarring who took part in our department's camouflage therapy workshop sessions during 2012. The workshops were given by specifically trained nursing staff and were originally intended for patients with scars from cancer surgery but later opened up to other patients of all ages whose facial skin conditions had a high quality-of-life impact.
The impact of each patient's skin condition on quality of life was assessed before the camouflage session and 2 weeks later, using the validated Spanish version of the Children's Dermatology Life Quality Index (cDLQI),9 a 10-item questionnaire that covers symptoms, influence on clothing choice, impact on athletics, and effect on friendships, whether at school time or during holidays.
Every item is scored from 0 to 3 according to how much it impacts the child's quality of life (0: not at all; 1: only a little; 2: quite a lot; 3: very much). The higher the total score (0–30), the higher the impairment.
The cDLQI was administered to assess quality-of-life impact and identify patients who might benefit from the camouflage therapy workshop. Then, the child attended a single camouflage session with an accompanying adult relative. Sessions included both makeup application and instruction, so that the patient could leave with the basic skills to carry out the task independently at home. Teaching points included the importance of skin cleansing and moisturization prior to makeup application, use of green to neutralize reddish lesions, and use of yellow/beige to neutralize hyperpigmented lesions.
The cosmetics used (Avène corrective makeup products) were hypoallergenic and water resistant, and frequently provided UV-A and UV-B protection.
Case DescriptionsWe reviewed 6 cases of patients aged 10 to 15 years. Most were girls (5 out of 6), and all, except for a 15-year-old boy with acne scarring, had pigmentary disorders. Each child had a single workshop session that included both instruction and makeup application. A family member was present so that both the child and the family could learn the basics and would be able to apply the cosmetics at home. A comparison of cDLQI scores showed a marked overall improvement in quality of life 2 weeks after the camouflage session. A follow-up telephone survey was conducted to assess changes 6 months after the session (Table 1).
Overall Improvement in Patient cDLQI After the Camouflage Session.
| N | Sex | Age | Skin Condition | No. of Sessions | cDLQI Before Session | cDLQI After Session | Cosmetic Camouflage Use After 6 Months |
| 1 | Female | 14 | Bilateral nevus of Ota | 1 | 14 | 6 | Independent use |
| 2 | Female | 11 | Hypomelanosis of Ito | 1 | 5 | 4 | None |
| 3 | Male | 15 | Acne scarring | 1 | 9 | 4 | Independent use |
| 4 | Female | 10 | Segmental vitiligo | 1 | 13 | 4 | Independent use |
| 5 | Female | 13 | Segmental vitiligo | 1 | 19 | 7 | Independent use |
| 6 | Female | 15 | Segmental vitiligo | 1 | 4 | 1 | Independent use |
Abbreviation: cDLQI, Children's Dermatology Life Quality Index.
A 14-year-old girl of South American origin had bilateral nevus of Ota that significantly impaired her quality of life. She was offered laser surgery, but given her dark skin (phototype V), the potential adverse effects, and the need to travel for the surgery, her parents declined this treatment. A camouflage therapy session was offered and proved satisfactory for both the patient and her family, significantly decreasing quality-of-life impairment (Fig. 1 A and B).
Case 2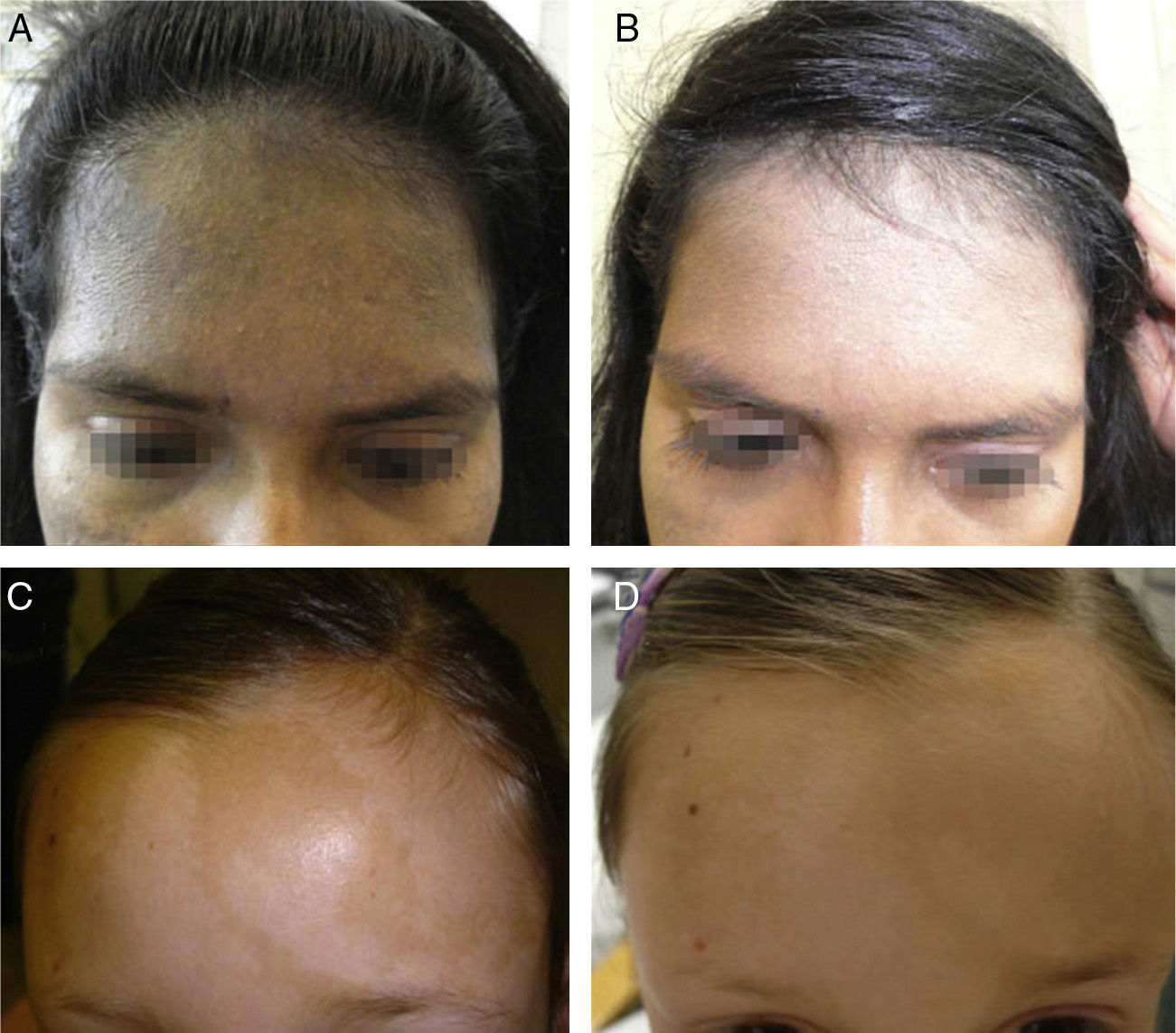
An 11-year-old girl with skin phototype II was being followed for mosaic hypopigmentation with facial involvement. Her previous quality of life was good. After the camouflage session concealed her facial lesions, the family felt that slight improvement had been achieved. After 2 weeks, the mother acknowledged a good cosmetic outcome but chose to wait and see, postponing use of makeup until the patient herself requested it (Fig. 1 C and D).
Case 3An adolescent male with skin phototype III had completed isotretinoin treatment and requested help in making his scars less visible. After his session, the result was considered acceptable. His parents also expressed considerable satisfaction (Fig. 2 A and B).
Case 4
A 10-year-old Moroccan girl with skin phototype IV had predominantly facial vitiligo involving the chin and an eyebrow. After the cosmetic camouflage session, both the child and her parents were very pleased with the outcome (Fig. 2 C and D).
Case 5An adolescent girl of Asian origin with skin phototype III had vitiligo on both eyelids, slightly affecting her quality of life. She used the camouflage advice daily and achieved a good cosmetic outcome. This patient attended her session on her own (Fig. 3 A and B).
Case 6
A 14-year-old girl of South American origin with skin phototype IV had predominantly facial vitiligo that failed to respond to topical treatment and narrowband UV-B phototherapy, much to the detriment of her quality of life. The result of the camouflage session was better than expected, and was considered acceptable by her parents both during the session itself and at follow-up (Fig. 3 C and D).
DiscussionCosmetic camouflage is useful in managing predominantly facial skin conditions in pediatric patients, particularly when medical and surgical treatments are ineffective or access to therapy presents difficulties.10
In childhood and during the critical adolescent years, certain skin disorders can significantly impair the patient's physical and psychological health. In fact, it has been widely reported that adolescent patients with vitiligo and/or acne are more likely to develop depression, loss of self-esteem, emotional distress, and body dysmorphic disorder.1 For these patients, corrective cosmetics can be of great help in minimizing the impact on quality of life.11,12
Cosmetic camouflage is a simple, cheap, noninvasive, and easily repeated procedure that serves as a complement rather than a replacement for definitive treatment.
While it is widely used by adult patients, mainly to conceal scarring from cancer surgery, its use in children is exceptional. The largest pediatric series published so far consisted of 15 patients (7–16 years) who achieved a satisfactory response in every case, with improved quality of life after the camouflage workshop.13 All our patients also experienced some mitigation of the impact of their skin conditions on their lives, to a greater or lesser degree.
The best cosmetic results are achieved with three types of skin conditions. Inflammatory conditions such as acne and rosacea are addressed by neutralizing reddish lesions with green hues and can also benefit from the antiinflammatory agents included in many of these products. Scarring and vascular abnormalities can be camouflaged with compact foundation that matches the patients’ skin phototype. Last but not least, pigmentation anomalies, particularly vitiligo, whose psychological impact is great, benefit the most from the use of corrective cosmetics.14,15
In summary, cosmetic camouflage can be a useful option for pediatric patients with skin conditions that cause both physical and psychosocial impairment.
Ethical DisclosuresProtection of human and animal subjectsThe author declares that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have followed their hospital's protocol on the publication of data concerning patients and that all patients included in the study have received sufficient information and have given their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no private patient data are disclosed in this article.
Please cite this article as: Padilla-España L, del Boz J, Ramírez-López M, Fernández-Sánchez M. Taller de camuflaje terapéutico en dermatología pediátrica: revisión de 6 casos 2014;105:510–514.


