

Sarcomas with BCOR genetic alterations, previously called Ewing-like sarcomas, are undifferentiated neoplasms of bone and soft tissues that share morphological characteristics with Ewing sarcoma but do not exhibit the classic molecular alterations of these tumors.1
A 12-year-old male, with no significant past medical history, was seen in the Dermatology Service with a 2-month history inflammatory and painful lesion located on the fifth toe of the left foot. On physical examination, an exophytic nodule was noted, causing digital deformity along with loss of the nail apparatus (Fig. 1).1
 Tumor of the fifth toe with acquired anonychia. (B) Exophytic growth 2 weeks after the first photograph.1")
(A) Tumor of the fifth toe with acquired anonychia. (B) Exophytic growth 2 weeks after the first photograph.1
A simple X-ray revealed increased soft tissue, deformity, and small-sized lytic areas. MRI revealed the presence of a 30mm×23mm×18mm lesion involving the distal and middle phalanges, with signs of bone infiltration, a multilobulated appearance, intermediate-low signal on T1, homogeneous hyperintensity on T2, and marked gadolinium uptake.
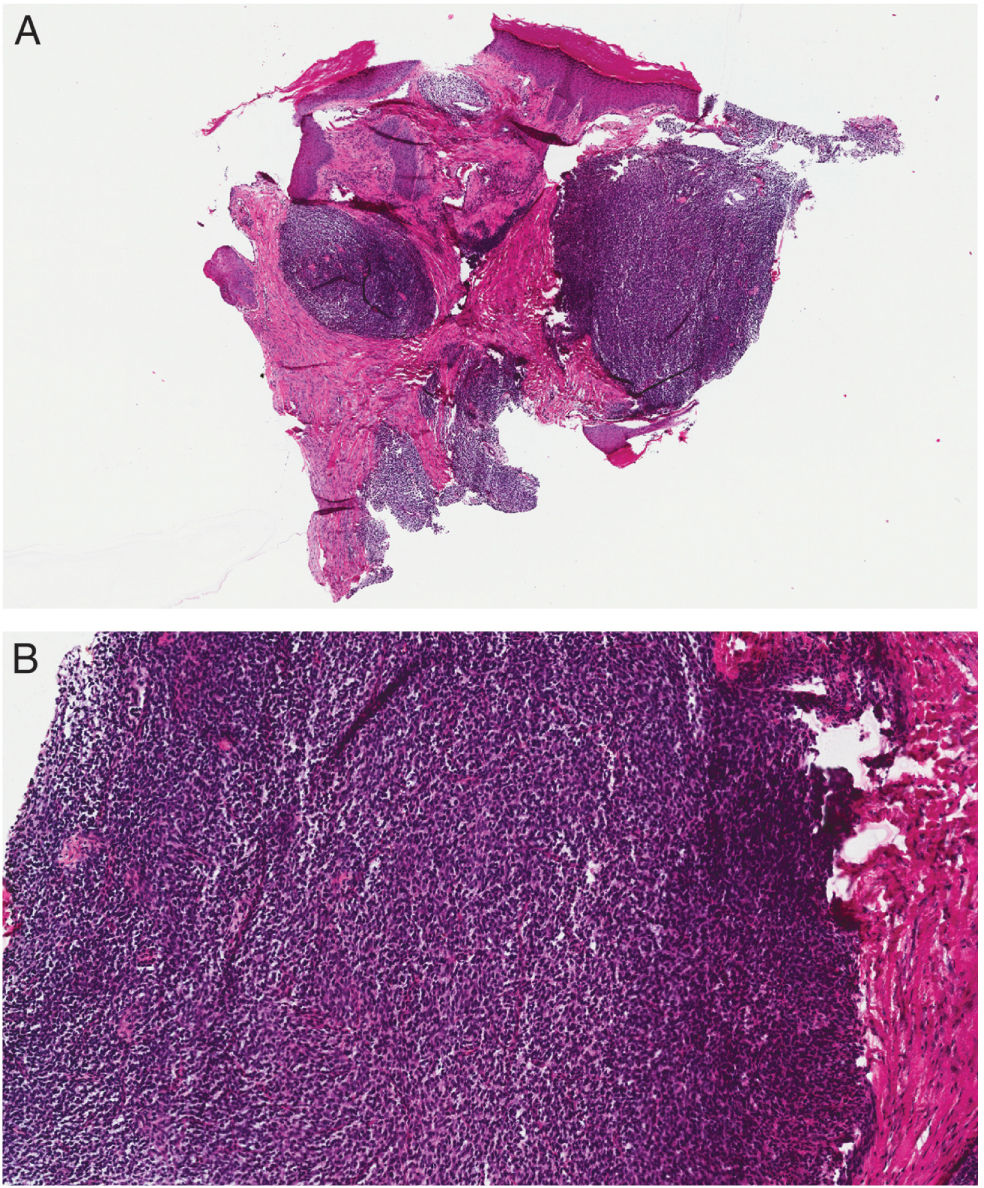
A biopsy of the lesion revealed an undifferentiated neoplastic proliferation with a sheet-like growth pattern. The cells were small and round or slightly fusiform in shape, with hyperchromatic nuclei and occasional mitoses (Fig. 2). The immunohistochemical study tested positive for vimentin, dot-like for CD99, and showed patchy positivity for BCOR. Fluorescence in situ hybridization (FISH) tested negative for EWSR1 and SYT, ruling out Ewing sarcoma and synovial sarcoma, respectively.
 Panoramic view showing a neoplastic infiltrate in a sheet-like pattern (H–E, 40×). (B) Detail of the infiltrate, composed of small round cells with hyperchromatic nuclei (H–E, 200×).2")
(A) Panoramic view showing a neoplastic infiltrate in a sheet-like pattern (H–E, 40×). (B) Detail of the infiltrate, composed of small round cells with hyperchromatic nuclei (H–E, 200×).2
Targeted sequencing using reverse-transcription polymerase chain reaction (RT-PCR) detected the BCOR-CCNB3 gene fusion.
After establishing the diagnosis of BCOR genetic alteration sarcoma, the left fifth toe was amputated and disarticulated, followed by 9 cycles of chemotherapy with vincristine, doxorubicin, and cyclophosphamide. The patient remained in complete remission 18 months after completing treatment.
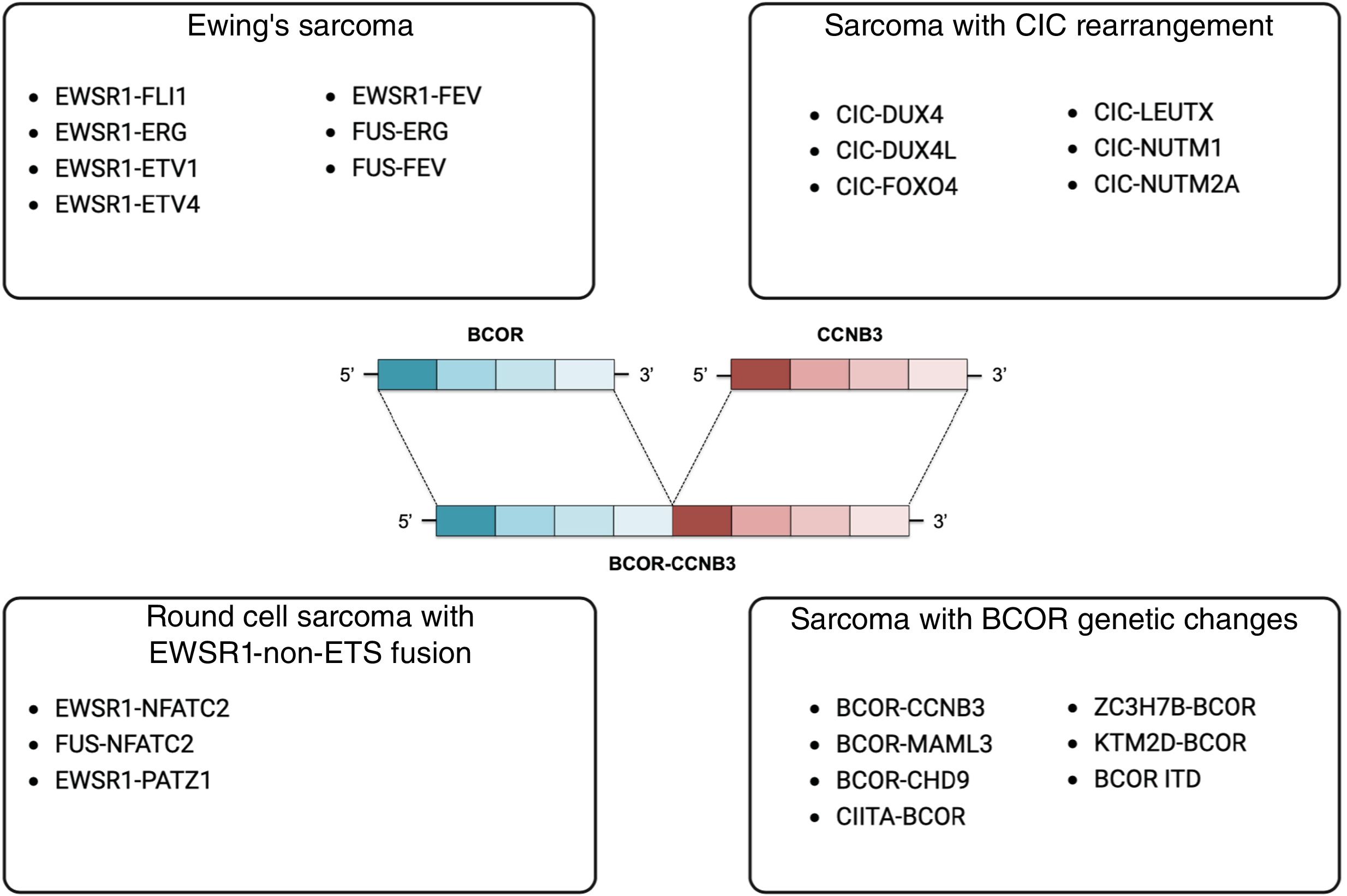
The 5th edition of the World Health Organization classification of soft tissue and bone tumors, from 2020, includes a new chapter titled “Undifferentiated Round Cell Sarcomas of Bone and Soft Tissue,” which categorizes 4 subtypes of tumors: Ewing sarcoma, sarcoma with CIC rearrangement, round cell sarcoma with EWSR1-no ETS fusion, and sarcoma with BCOR genetic alterations (Fig. 3).2

Diagram showing the gene fusions of undifferentiated small round cell sarcomas of bone and soft tissue characterized to date. In the center, representation of the BCOR-CCNB3 fusion present in our patient.3
Ewing sarcoma typically appears in the diaphysis of long bones, ribs, and pelvis, though 10% of cases are extraskeletal. These tumors are more common in patients under 20 years of age, while older patients tend to present Ewing sarcomas in soft tissues. All cases exhibit the fusion of EWSR1 or FUS genes with ETS family transcription factors, with the most common fusions being EWSR1-FLI1 (85%) and EWSR1-ERG (10%).3,4
The other 3 subtypes of round cell sarcomas, known as Ewing-like sarcomas, have similar clinical and morphological characteristics but lack the previously described classic fusions.
CIC-rearranged sarcoma occurs primarily in deep soft tissues of the trunk and limbs, occasionally in the viscera or bone. It affects patients across a wide age range. In 95% of cases, the CIC-DUX4 gene fusion is detected, although isolated cases of CIC fusions with FOXO4, LEUTX, NUTM1, and NUTM2A have also been described.4,5
Round cell sarcoma with EWSR1-non-ETS fusion is a very rare subgroup of sarcomas that present EWSR1-NFATC2, FUS-NFATC2, and EWSR1-PATZ1 fusions. The age range is variable, and these tumors mainly appear in the metaphyses and diaphyses of long bones, with lesser involvement of soft tissues of the trunk and limbs. The FUS-NFATC2 fusion has only been described in bone sarcomas.4,6
BCOR genetic alteration sarcoma is slightly more prevalent in soft tissues than in bone, with a predilection for the pelvis and lower limbs. The most common BCOR-CCNB3 fusion occurs in more than 90% of cases in males under 20 years of age.7 Less common fusions with MAML3 and ZC3H7B occur in older patients. Tandem internal duplications of BCOR may be congenital or develop within the first year.1,4 Histologically, in addition to the round cell morphology, this subgroup is characterized by the presence of fusiform-shaped cells and focal or patchy immunohistochemical positivity for BCOR.7
Treatment for round cell sarcomas involves local surgery or radiotherapy on the lesion, followed by classic chemotherapy regimens for Ewing sarcoma.5
Due to the low incidence of these sarcomas, their knowledge is important in helping with early diagnosis and referral to specialized centers where multidisciplinary management is provided.
FundingNone declared.



