



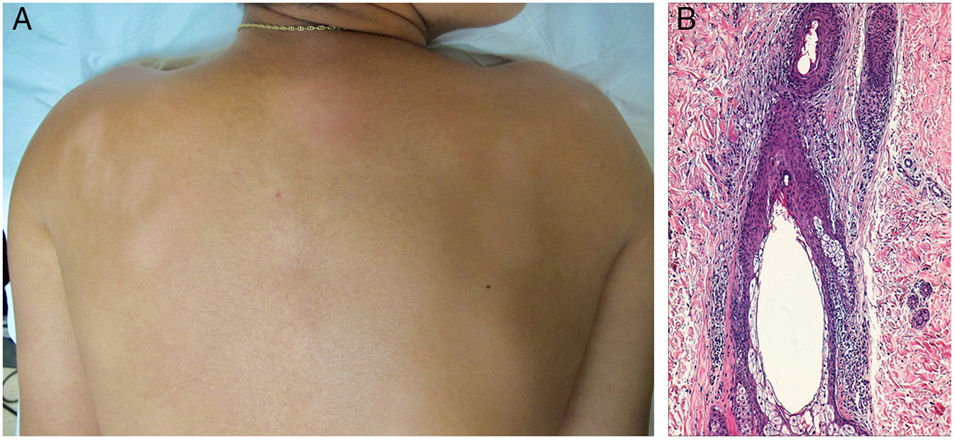
A 14-year-old boy presented with oval-shaped patches of hypopigmented alopecia and hypoesthesia on the back, legs, and forearms, which had appeared 9 months earlier (Fig. 1A). Tests ordered included a complete blood count, biochemistry, antinuclear antibodies, immunoglobulin, and protein electrophoresis in addition to a Mantoux test and serology for syphilis, HIV, hepatitis B virus, and hepatitis C virus. All test results were normal or negative. Polymerase chain reaction (PCR) on a skin biopsy sample was negative for Mycobacterium leprae. Histologic findings included a chronic but moderate lymphocytic inflammatory infiltrate without atypia in a panfollicular and folliculocentric distribution, with discrete spongiosis and no lichenoid damage (Fig. 1B). Colloidal iron staining revealed a slight mucin layer in the follicular epithelium. The lymphocytic infiltrate was composed almost entirely of T cells. Immunostaining was diffuse for CD4, CD3, CD5, and CD8 and focal for CD20. No monoclonal rearrangement was detected (after PCR) for the T-cell receptor gene. The lesions resolved spontaneously.
Some authors consider mucin-poor follicular mucinosis—also known as folliculotropic T-cell lymphocytosis—to be a variant of cutaneous lymphoid dyscrasia with a low risk of progression to cutaneous T-cell lymphoma. As happened in our case, hypoesthesia or dysesthesia is not an uncommon finding in mucinous alopecia lesions. The cause of hypoesthesia in mucinous alopecia is unclear, but it is thought that much of the cutaneous innervation is associated with the hair follicle and surrounding vascularization. When these structures are severely affected, sensitivity is altered. In cases like this one, the principal differential diagnosis is the folliculotropic variant of hypopigmented mycosis fungoides.
Please cite this article as: Monteagudo B, Vázquez-Bueno JÁ, León-Muiños E. Alopecia e hipoestesia en linfocitosis de células T foliculotrópica. Actas Dermosifiliogr. 2019;110:e2.


