




Local anesthetics are widely used in clinical practice, and adverse effects are not uncommon. Delayed hypersensitivity reactions are among the most common effects, but immediate-type reactions may also occur. Patch testing should be considered in patients with hypersensitivity reactions. We present a case of allergic contact dermatitis to benzocaine that was detected incidentally by patch testing and highlight the importance of correctly interpreting patch test results when there are concomitant positive reactions.
Los anestésicos locales son fármacos ampliamente utilizados en la práctica clínica. Los efectos adversos asociados a su uso no son infrecuentes, y las reacciones de hipersensibilidad retardada se encuentran entre los más habituales, aunque también están implicadas las reacciones de hipersensibilidad inmediata. En estos casos debe considerarse la realización de pruebas de alergia cutánea. Presentamos un caso de alergia de contacto a la benzocaína detectada de manera incidental mediante pruebas epicutáneas, que ilustra la importancia de realizar una correcta interpretación de los resultados positivos concomitantes en todos los casos.
Local anesthetics are widely used drugs. Their adverse effects are frequent and can be caused by immediate-type or delayed hypersensitivity reactions. Topical products containing anesthetics are increasingly applied and have the potential to cause allergic contact dermatitis. Skin testing for allergy should always be considered in such cases. We present a case of skin allergy to benzocaine that was detected incidentally by patch testing.
Case DescriptionThe patient was a 53-year-old homemaker who was referred to the allergy unit of our dermatology department with a 2-year history of blepharitis consisting of highly pruritic, scaly, erythematous plaques on both upper eyelids that had been successfully treated with topical corticosteroids. She had no personal or family history of atopy, allergy, or psoriasis. When the history was taken, no other skin lesions were visible and the patient was unable to identify a trigger.
We performed patch tests according to the recommendations of the Spanish Contact Dermatitis and Skin Allergy Research Group (GEIDAC) with its standard series (TRUE Test, provided by Martí Tor), toluenesulfonamide formaldehyde resin 10% in petrolatum (pet) (included in the plastics and glues series of Martí Tor), and the patient's facial moisturizing cream as she applied it at home (tested using Finn chambers). Patches were applied to the upper back and readings were taken at 48 and 96hours, according to the guidelines of the International Contact Dermatitis Research Group. The results were positive for methylchloroisothiazolinone/methylisothiazolinone 100ppm in aqueous solution (aq), caine mix (dibucaine 1%, tetracaine 1%, and benzocaine 5% pet), paraphenylenediamine (PPD) 1% pet, and the patient's cream (Table 1). The results obtained for methylchloroisothiazolinone/methylisothiazolinone and the moisturizing cream were considered to have present relevance, although we were unable to test the individual components of the cream. The positive results to caine mix or PPD were not initially found to have present relevance.
Results of Patch Tests at 48 and 96 Hours.
| Allergen | 48h | 96h |
| Methylchloroisothiazolinone/methylisothiazolinone 100ppm aq | + | ++ |
| Caine mix (dibucaine 1%, tetracaine 1%, and benzocaine 5% pet) | ++ | ++ |
| Paraphenylenediamine 1% pet | - | + |
| Toluenesulfonamide formaldehyde resin 10% pet | - | - |
| Patient's facial cream | ++ | ++ |
| Benzocaine 5% pet | + | ++ |
Abbreviations: aq, aqueous solution; pet, petrolatum.
These findings, however, led us to extend the study using a local anesthetics series (Martí Tor), which yielded positive results to caine mix (D2+/D4++) and benzocaine 5% (D2+/D4++). After further questioning, the patient reported an episode of edema on the left side of her face followed by dyspnea 14hours after a tooth extraction. During the procedure, benzocaine 20% gel (Hurricaine gel; Laboratorios Clarben S.A.) was applied to the oral mucosa before an injection of local anesthetic with mepivacaine 2%. The episode resolved only after parenteral administration of corticosteroids.
The patient was referred to the allergology department to undergo skin tests and challenge tests with local anesthetics (lidocaine, bupivacaine, and mepivacaine) and skin tests with latex. The results to all the tests were negative.
The lesions on the eyelids improved after withdrawal of the moisturizing cream and avoidance of products containing methylchloroisothiazolinone/methylisothiazolinone.
Our findings confirmed a diagnosis of contact sensitization to benzocaine and blepharitis caused by contact with cosmetic products.
DiscussionBenzocaine is an ester local anesthetic. Introduced in 1902, it was the first synthetic agent composed of the ethyl ester of para-aminobenzoic acid to be used in clinical practice.1 It interacts with the sodium channels of the cell membrane to block local nerve impulses. It is absorbed in very small quantities by the membrane and is hydrolyzed by plasma pseudocholinesterases (and much less so by liver cholinesterases) to metabolites that contain para-aminobenzoic acid, which is highly allergenic and responsible for anaphylactic reactions. The risk of reaction is greater in patients with altered enzyme function. Benzocaine is eliminated primarily by the kidneys, mainly as inactive metabolites.
In Spain, benzocaine is marketed for topical administration. It is used in the manufacture of various products to reduce pain, itching, or burning sensation associated with abrasions, actinic burns, insect stings, toothache, and leg ulcers. It is also found in antihemorrhoidal creams, some oral suspensions, and cough tablets and can be applied topically to the oral mucosa during dental procedures before injection of local anesthetic.
The literature contains few reports on allergy to anesthetics. Nevertheless, allergic reactions to local anesthetics are frequent. Amide anesthetics (mepivacaine, bupivacaine, lidocaine, and prilocaine) are better tolerated, whereas ester anesthetics (benzocaine, procaine, tetracaine, and chloroprocaine) are more allergenic. Among the latter, benzocaine yields the greatest number of positive results in patch tests.2 Moreover, patients with allergy to ester anesthetics can tolerate amide anesthetics, and vice versa. In the few reported cases of positive results to both groups of anesthetics, the reaction seems more likely to be concomitant sensitization than a cross-reaction between them.3,4
It has been estimated that 5% of patients who use topical preparations of benzocaine become sensitized to it; therefore, long-term use can lead to the appearance of hypersensitivity reactions (<1% of all adverse reactions).5,6 Most are T cell–mediated type IV delayed hypersensitivity reactions involving contact dermatitis that are confirmed by patch tests.6–8 Other types of hypersensitivity reaction (type I), namely, immunoglobulin E–mediated immediate-type reactions (e.g., urticaria, angioedema, or anaphylaxis) are extremely rare.9
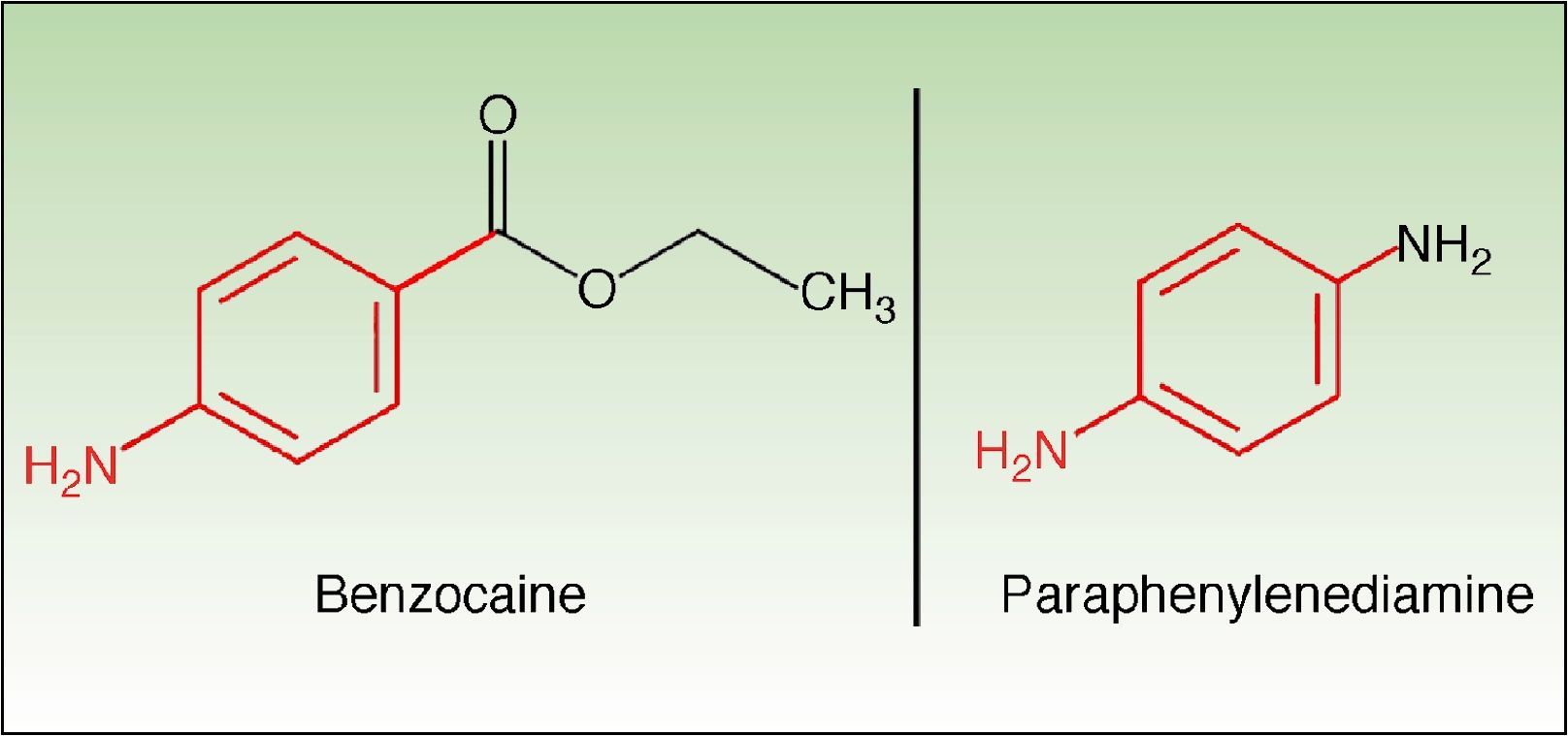
Benzocaine can cross-react with several allergens. Possible explanations for this phenomenon include the presence of common antigenic determinants or transformation to chemically related metabolites in the skin. Benzocaine, parabens, PPD, 2,5-diaminotoluene sulfate, 2-nitro 1,4-PPD, and the azo dyes used in textiles belong to the same group. They have in common the presence of an amino substituent at the para position of the benzene ring. This structural similarity could explain the frequency of cross-reactions, such as that observed in our patient between PPD and benzocaine (Fig. 1).10
In conclusion, we have presented a case of cutaneous allergy to benzocaine that was detected incidentally and confirmed by positive patch test results in a patient referred with longstanding blepharitis. The patient had previously presented with an episode of edema on the left side of her face associated with topical application of benzocaine.
We recommend that the standard series contain caine mix instead of benzocaine alone, since it enables us to detect most reactions to benzocaine and to screen for other common anesthetics, for example, tetracaine, which is found in products such as urinary catheter lubricants, stoma lubricants, and antihemorrhoidal creams.
Similarly, we stress the importance of taking a meticulous history in order to ensure correct diagnosis and interpretation of the skin test results, with special emphasis on concomitant positive results, since their repercussions for the patient can be serious.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: González-Rodríguez AJ, et al. Alergia de contacto a benzocaína. Importancia de los resultados positivos concomitantes en las pruebas epicutáneas. Actas Dermosifiliogr. 2013;140:156–8.


