


Cutaneous metastasis is the clinical manifestation of neoplastic cells that have spread to the skin from a visceral tumor. Its prevalence, which is rising due to higher rates of histologic diagnosis and/or evaluation, is estimated at between 0.7% and 9% depending on the series.1 Cutaneous metastases are a common reason for consultation between dermatologists and are often suspected as an initial diagnosis because the lesions are easily identifiable during physical examination. They are important to recognize as they can lead to the diagnosis of an unknown primary tumor, indicate the spread of a known tumor, or be an early sign of recurrence of a tumor thought to be in remission.2 The most common visceral tumors that cause cutaneous metastasis are lung cancer in men, breast cancer in women, and gastric adenocarcinomas in both men and women.3 Cutaneous metastases can present as any number of elementary lesions, which can be solitary or multiple or asymptomatic or painful.
Diagnosis must be confirmed histologically and in some cases an immunohistochemical panel may be necessary. Few studies and case series have analyzed the value of imaging studies prior to biopsy in cutaneous metastasis. High-frequency skin ultrasound is a fast, safe technique that can provide diagnostic information and, on occasions, preoperative information following a clinical diagnosis. Findings often lead to a change in disease stage.
We present 6 cases of cutaneous metastasis from visceral tumors evaluated in our department between January and July 2017. We describe clinical and epidemiological characteristics and B-mode and Doppler ultrasound features. All the metastases were studied using the Esaote Mylab ultrasound system equipped a transducer that operates between 18 and 20MHz. The Doppler pulse repetition frequency was 750MHz for a 20-MHz frequency, and the gain was adjusted to the level immediately before the flash artifact.
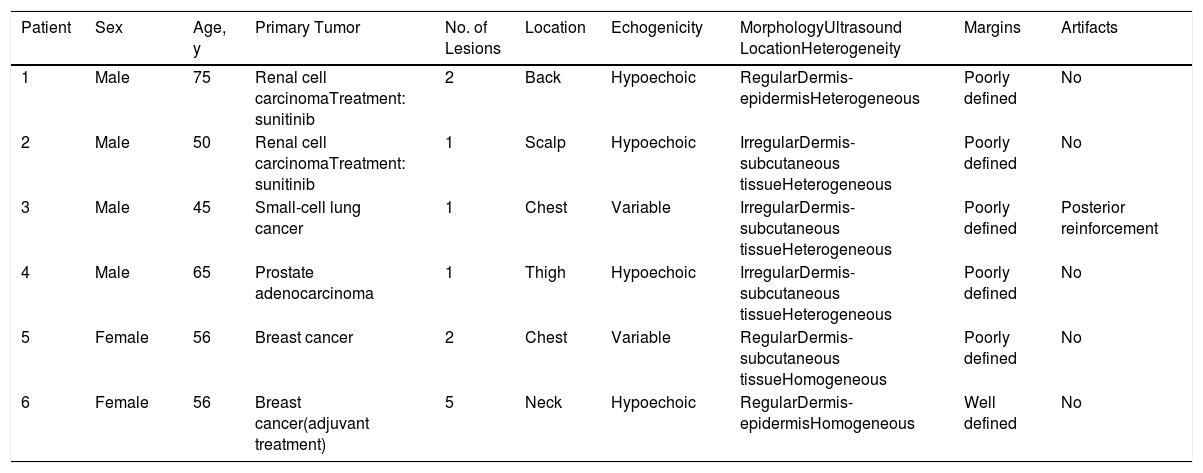
There were 4 men and 2 women aged between 45 and 75 years. All the patients were referred to the medical oncology department for evaluation of skin lesions suspected to be cutaneous metastases. Just 1 patient was receiving adjuvant therapy. The other 5 were under treatment for a previously diagnosed tumor. Three of the patients had just 1 lesion when evaluated by the dermatology department. All the lesions had a diameter of over 9mm except for some smaller lesions (4-6mm) in patient #6. The epidemiologic, clinical, and B-mode ultrasound characteristics are summarized in Table 1.
Epidemiological, Clinical, and Ultrasound Characteristics in 6 Patients With Cutaneous Metastases From Visceral Tumors.
| Patient | Sex | Age, y | Primary Tumor | No. of Lesions | Location | Echogenicity | MorphologyUltrasound LocationHeterogeneity | Margins | Artifacts |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 75 | Renal cell carcinomaTreatment: sunitinib | 2 | Back | Hypoechoic | RegularDermis-epidermisHeterogeneous | Poorly defined | No |
| 2 | Male | 50 | Renal cell carcinomaTreatment: sunitinib | 1 | Scalp | Hypoechoic | IrregularDermis-subcutaneous tissueHeterogeneous | Poorly defined | No |
| 3 | Male | 45 | Small-cell lung cancer | 1 | Chest | Variable | IrregularDermis-subcutaneous tissueHeterogeneous | Poorly defined | Posterior reinforcement |
| 4 | Male | 65 | Prostate adenocarcinoma | 1 | Thigh | Hypoechoic | IrregularDermis-subcutaneous tissueHeterogeneous | Poorly defined | No |
| 5 | Female | 56 | Breast cancer | 2 | Chest | Variable | RegularDermis-subcutaneous tissueHomogeneous | Poorly defined | No |
| 6 | Female | 56 | Breast cancer(adjuvant treatment) | 5 | Neck | Hypoechoic | RegularDermis-epidermisHomogeneous | Well defined | No |
Large series have reported on the ultrasound features of cutaneous metastases from melanoma,4 but this has not been the case for metastases from visceral tumors.5,6 Moreover, most of the series that do exist have been published by radiologists and deal mainly with subcutaneous lesions (both palpable and nonpalpable). The authors of these studies stress that while cutaneous metastases do not necessarily indicate terminal disease, they are always a sign of disease spread. From an ultrasound perspective, all the lesions studied were located in the subcutaneous tissue, whereas in our series, given their accessibility, they were also observed in the epidermis and dermis. The most characteristic B-mode ultrasound finding for metastatic cutaneous lesions is an irregular, polycyclic shape, which was observed in 5 of the 6 patients in our series (Fig. 1).

Giovagnario et al.7 described 4 vascular patterns for cutaneous metastases evaluated by ultrasound: avascular, hypovascular with a single vascular pole, hypervascular with multiple peripheral poles, and hypervascular with internal vessels. All 4 patterns were observed in our series. Some authors have claimed that vascularization is highly suggestive and predictive of malignancy, with a sensitivity of 91% and a specificity of 93%.8 Avascular and hypovascular patterns may be due to lesion size, necrosis, or the presence of vessels that are too small to detect with the equipment used. This was the case with patient #6 in our series (Fig. 2).

In conclusion, we have described the ultrasound features of a series of cutaneous metastases from visceral tumors with similar clinical features to those described in the literature. B-mode ultrasound does not reveal any specific patterns and must be complemented by Doppler imaging, which offers greater diagnostic sensitivity and specificity. High-frequency skin ultrasound is a useful diagnostic method for planning treatment and monitoring cutaneous metastases from visceral tumors.
Please cite this article as: Cuenca-Barrales C, Aguayo-Carreras P, Bueno-Rodriguez A, Ruiz-Villaverde R. Estudio ecográfico de metástasis cutáneas de origen visceral. Actas Dermosifiliogr. 2019;110:506–509.


