

The world is in constant change, and dermatology is no exception. Present or future?
It is a proven fact that dermatologists are increasingly expanding their scope of action, adding different procedures and techniques into their routine clinical practice, which has further enriched this field of medicine.1,2
We have several examples of this such as surgical oncology through the performance of large flaps; trichology with its mesotherapy techniques, and hair transplant; lasers and light sources, as well as aesthetic dermatology with the use of fillers and botulinum toxin as anti-aging techniques.3
Nonetheless, this does not mean that more traditional areas of our specialty have been left aside, such as inflammatory disease represented by psoriasis, atopic dermatitis, or hidradenitis suppurativa, which by the way, are also on the rise due to the emergence of new biologic drugs or molecules such as the JAK inhibitors; oncology represented by melanoma, non-melanoma skin cancer, and lymphomas; and venereology with classic entities such as syphilis and latest additions such as Monkeypox.4
But how does the professional field actually look like? The current scenario can be summarized as follows: on one hand, a public health care system with a growing demand for services that continues to offer precarious contracts to its workers; on the other, private clinics and large hospital and health systems continue to grow making all kinds of technologies and resources available to be able to practice comprehensive dermatology, which is better paid and offers better conditions to balance work with family life. Therefore, with an “almost infinite” possibility of subspecialization, making a decision on their professional future is challenging for residents and young assistant physicians.5
To understand the concerns and future job prospects of residents from the Spanish Academy of Dermatology and Venereology (AEDV), an online survey was sent to 183 people out of 380 participants, which means that 48.1% of all dermatology residents in Spain responded to the survey.
A total of 78 men (42.6%) and 105 women (57.4%) responded to the survey, with participation being distributed as follows:
By territorial sections: Central Section, 24%; Andalusian section, 13.7%; Basque-Navarrese-Aragonese-Riojan and Catalan section, 12%; Valencian section, 10.9%; Asturian-Cantabrian-Castilian-Leonese, 10.4%.
By year of residency: 43 (23.5%), 59 (32.2%), 44 (24%), and 37 (20.2%) residents were 1st, 2nd, 3rd, and 4th year residents, respectively.
Based on their “ideal” job destination after completing their residency, a total of 3 subgroups were identified: public health care, private sector, or mixed public-private system (table 1).
In the public health care group, the prevailing idea is to have a specialized clinic in the hospital, along with a general practice in a specialty center (63.2%), followed by the idea of practicing only in specialized clinics (42.1%). Regarding subspecialization, the field of autoimmune disease is the most popular one in this group (57.9%), followed by oncology (42.1%), and to a lesser extent, surgery, inflammatory disease, and pediatrics. Regarding teaching, 79% would like to be a full/associate professor in a public university, while there is also interest in training candidates for the MIR exam or participating in training courses (table 2).
A total of 8 participants responded from the group with a more entrepreneurial, or private health care-oriented profile. Among them, 3 would like to have their own clinic, 4 would rather work in a dermatology group with other colleagues, and none would like to work in a private hospital seeing patients from insurance companies. In addition, they would focus their clinical dermatology practice (from most to least interesting) on aesthetic dermatology, laser, trichology, and surgery. However, they would not want to abandon teaching, as 5 of them would like to become professors in a Master's Degree in Dermatology or participate in educational activities.
The mixed public-private modality combining the 2 previous options was the most successful group, with a total of 145 residents. They were asked how they would distribute their time between the two. Seventy-six respondents (52.4%) said they would like to work in the public health care system with contracts covering 50% of their regular working hours (17.5-20hours/week depending on the autonomous community) complementing the other 50% working in the private health care system vs only 9 people (40.7%) who would rather work 75% of their time in the public health care system, with only 25% of their working hours dedicated to the private sector. Details on teaching and subspecialization for this group are shown in tables 2 and 3.
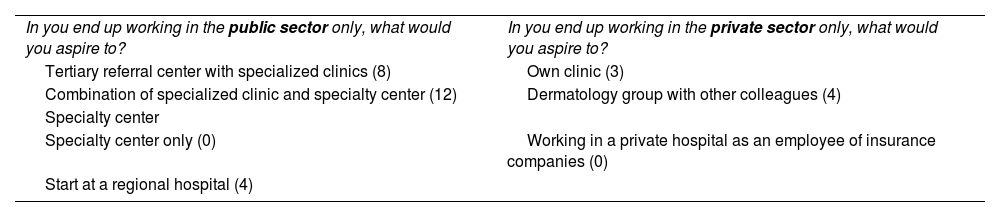
Expectations regarding working options in the public and private sectors.
| In you end up working in the public sector only, what would you aspire to? | In you end up working in the private sector only, what would you aspire to? |
| Tertiary referral center with specialized clinics (8) | Own clinic (3) |
| Combination of specialized clinic and specialty center (12) | Dermatology group with other colleagues (4) |
| Specialty center | |
| Specialty center only (0) | Working in a private hospital as an employee of insurance companies (0) |
| Start at a regional hospital (4) |
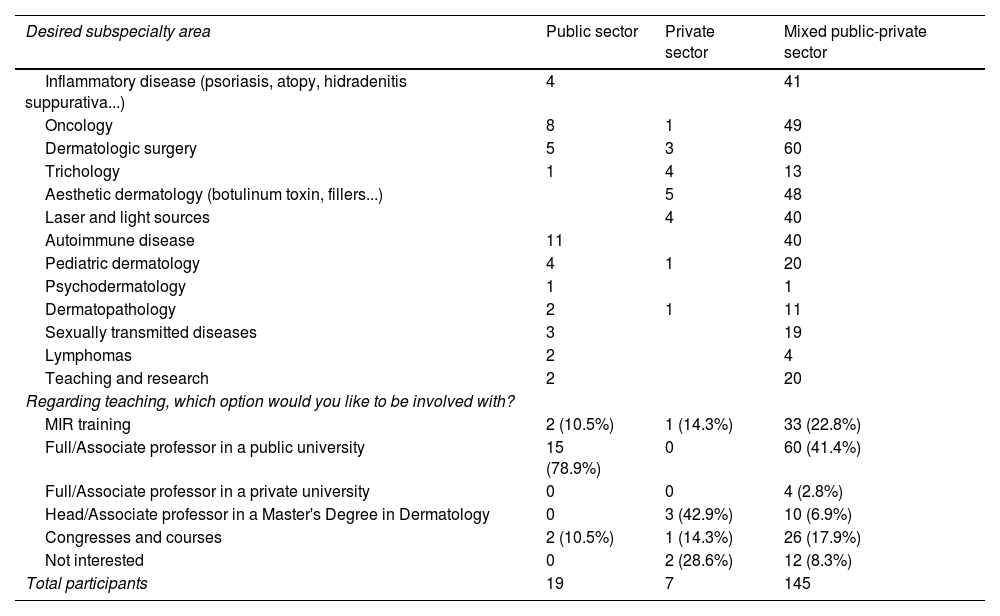
Subspecialization among different groups and teaching.
| Desired subspecialty area | Public sector | Private sector | Mixed public-private sector |
|---|---|---|---|
| Inflammatory disease (psoriasis, atopy, hidradenitis suppurativa...) | 4 | 41 | |
| Oncology | 8 | 1 | 49 |
| Dermatologic surgery | 5 | 3 | 60 |
| Trichology | 1 | 4 | 13 |
| Aesthetic dermatology (botulinum toxin, fillers...) | 5 | 48 | |
| Laser and light sources | 4 | 40 | |
| Autoimmune disease | 11 | 40 | |
| Pediatric dermatology | 4 | 1 | 20 |
| Psychodermatology | 1 | 1 | |
| Dermatopathology | 2 | 1 | 11 |
| Sexually transmitted diseases | 3 | 19 | |
| Lymphomas | 2 | 4 | |
| Teaching and research | 2 | 20 | |
| Regarding teaching, which option would you like to be involved with? | |||
| MIR training | 2 (10.5%) | 1 (14.3%) | 33 (22.8%) |
| Full/Associate professor in a public university | 15 (78.9%) | 0 | 60 (41.4%) |
| Full/Associate professor in a private university | 0 | 0 | 4 (2.8%) |
| Head/Associate professor in a Master's Degree in Dermatology | 0 | 3 (42.9%) | 10 (6.9%) |
| Congresses and courses | 2 (10.5%) | 1 (14.3%) | 26 (17.9%) |
| Not interested | 0 | 2 (28.6%) | 12 (8.3%) |
| Total participants | 19 | 7 | 145 |
In conclusion, this was just a snapshot of the current state of the “youngest” dermatology practice in Spain, which has the difficult task (and, also, the advantage, unlike previous professional times) of being able to choose from different career paths.
This study did not cover the needs, concerns, and future fields of action that will surely continue to make our specialty grow and enrich itself.
Conflicts of interestNone declared.



