



The 2 lesions were exophytic tumors situated on the face. In the first patient, the clinical diagnosis was of a malignant tumor with a broad differential diagnosis and, in the second, before dermoscopic examination, a diagnosis of atypical seborrheic keratosis was made (Fig. 1).

The dermoscopic examination of the most exophytic part of the lesion in the first case showed a predominance of scales and hemorrhagic crusts that made it difficult to view the underlying structures clearly. However, structures that might suggest the diagnosis could be seen, such as the presence of an atypical polymorphic vascular pattern and a milky-red area on the right side of the lesion in the image (Fig. 2A, at 3 o’clock). In addition, in the center of the lesion there was a homogeneous bluish area that could be taken as a blue-gray veil or may simply have been the result of bleeding into the tumor; it is difficult to be certain. In these cases it is important to try to observe the base of the lesion. With this aim, we performed dermoscopic photographs after rotating the camera inferiorly, in contact with the tumor, in order to view the base of the tumor, which can be seen in the upper part of the image (Fig. 2 and Fig. 3 A). In this area there is a clear pigment network, which is the archetypal dermoscopic structure of melanocytic lesions.1 In this way, after evaluating the base and considering the other dermoscopic signs, we could be sure that we were dealing with an invasive melanoma; this diagnosis was confirmed by the pathologist.
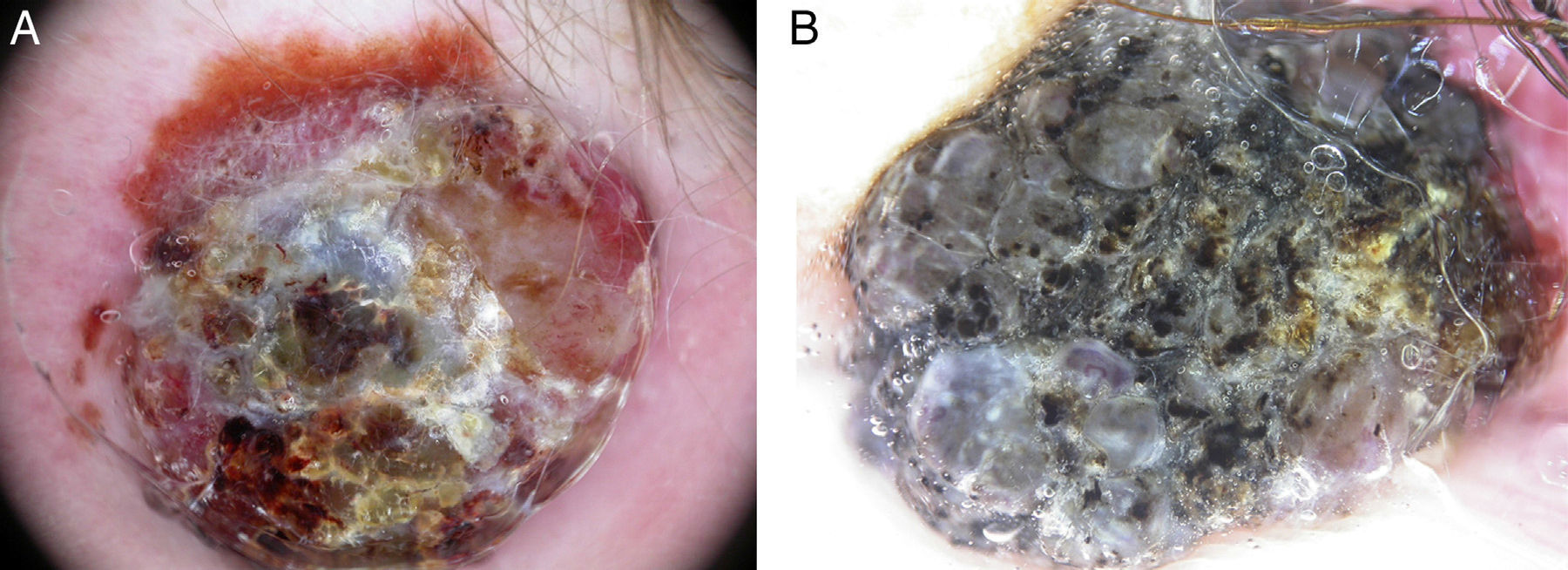
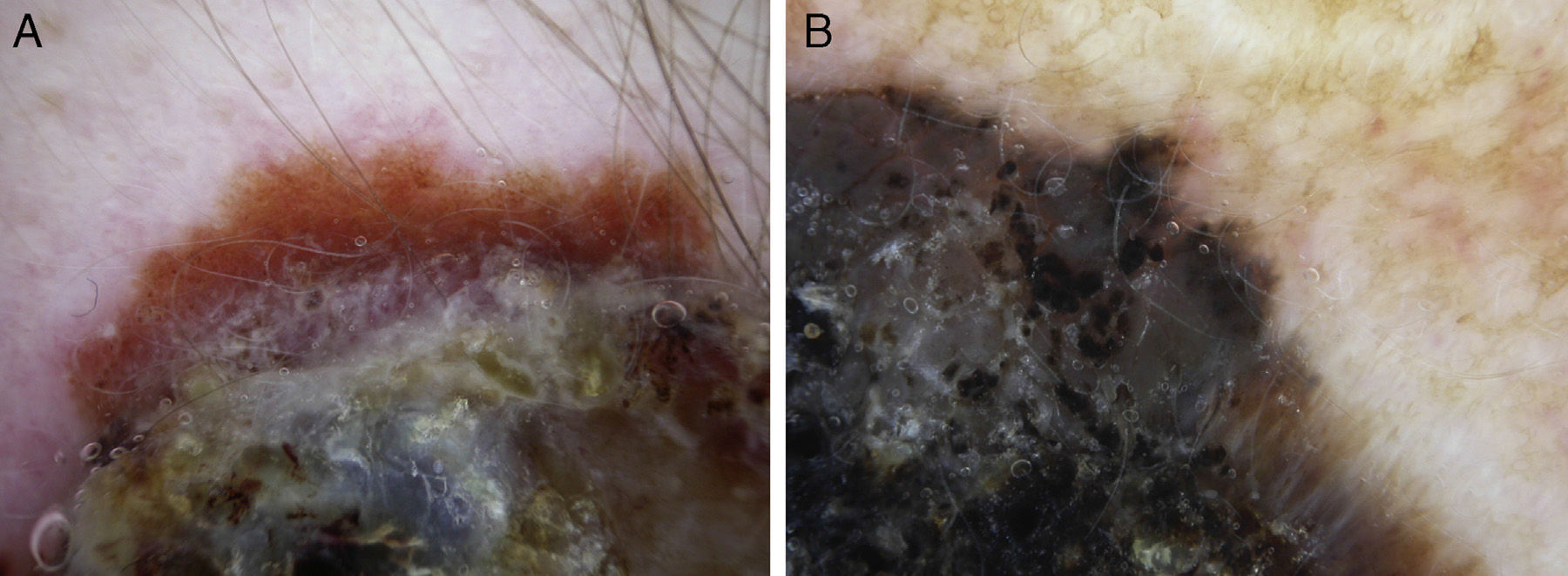
The dermoscopic image in the second case was very heterogeneous and disordered (Fig. 2B). There was an extensive area of scaling, keratosis, occasional comedo-like openings and a few possible milia-like cysts; without dermoscopy, these signs would point towards seborrheic keratosis as the suspected diagnosis. However, we also observed some homogeneous grayish structures that contained atypical blood vessels—not characteristic of seborrheic keratoses—and a probable milky-red area in the lower right part of the image (at 4-5 o’clock). In addition, aggregates of atypical dark brown globules were present in some areas (for example, at 9 o’clock on the image). The finding that gave us the dermoscopic diagnosis was again observed on evaluation of the base of the lesion. Apart from the aggregates of atypical dark brown globules and a possible blue-gray veil, peripheral streaks were also observed (Fig. 3B); these are one of the most characteristic features of melanocytic lesions.1 The tumor was excised with a diagnosis of nodular-verrucous melanoma, and this diagnosis was confirmed by the pathologist.
In conclusion, in highly exophytic lesions, many structures can be superimposed, leading to confusion and difficulty of interpretation. In such cases it can be very useful to evaluate the dermoscopic structures of the base of the lesion.
Please cite this article as: Zaballos Diego P. La raíz del problema. Actas Dermosifiliogr. 2014;105:712–713.



