








Child abuse is far more prevalent today than is generally recognized. Up to 90% of victims suffer physical abuse that can be observed in signs on the skin. Dermatologists are particularly qualified to identify these signs and distinguish them from other conditions that can mimic abuse. This review covers the signs of child abuse that can be observed on the skin. We discuss clues that can help differentiate between lesions caused by abuse and those that are accidental, and we describe the skin conditions that mimic physical abuse.
El maltrato infantil es mucho más frecuente de lo que generalmente se reconoce. Hasta el 90% de las víctimas que sufren maltrato físico presentan hallazgos cutáneos. El dermatólogo es el profesional más cualificado para identificar los signos cutáneos del maltrato y diferenciarlos de aquellas condiciones dermatológicas que puedan simularlo. En este artículo se revisan las manifestaciones cutáneas del maltrato infantil, indicando pistas que pueden ayudar al dermatólogo a discernir entre las heridas causadas por un maltrato y aquellas producidas accidentalmente, así como las condiciones dermatológicas que puedan imitarlo.
Although child abuse has existed since time immemorial, it was not until the American Pediatric Society meeting of 1959 that the term battered child syndrome was first used by Kempe and Silver, and subsequently published by Kempe et al.1 Since then, child abuse has attracted increasing attention from health care professionals, and particularly from pediatricians, who are especially aware of the problem and play a key role in its diagnosis, treatment, and, prevention. Child abuse, however, still receives limited attention from dermatologists, yet skin lesions resulting from physical abuse are the most visible manifestation of this major problem. It has been estimated that 50% of children who have been abused will be abused again and that 10% are at risk of death if the problem is not detected early.2 The role of the dermatologist in recognizing mucocutaneous signs suggestive of child abuse is fundamental.
Because of its violent, shameful nature, child abuse is underreported, and hence official statistics on the scope of this problem vary considerably. According to data from the United Kingdom and the United States, between 1% and 2% of children are abused every year. Furthermore, 1 in 1000 children is seriously injured and 1 in 10 000 dies from related injuries.3 Children under 4 years of age are at the greatest risk of severe injury, and 79% of fatalities resulting from abuse occur in this age group (44% in children under 1 year of age).4 Despite the work being done by child protective services, there is still a clear tendency towards an increase in the prevalence of child abuse. Between 1990 and 2004, the number of children evaluated for suspected abuse rose by 32.4%. According to a recent report by the Autonomous Government of Catalonia, child abuse is not confined to broken or dysfunctional homes. The report stated that 42% of child abuse cases occurred in intact, functional families and that in 80% of cases, the perpetrators were the children's parents.
There are many systems for classifying child abuse, but the most practical one is perhaps the clinical system. It recognizes 4 main types of abuse, which are, in decreasing order of frequency, neglect, physical abuse, sexual abuse, and emotional or psychological abuse. We will first discuss physical abuse, which is most often manifested through skin lesions.5 We will then review the main aspects of physical neglect and sexual abuse and provide useful clues for identifying and confirming suspected cases of child abuse.
Cutaneous Manifestations of Physical AbuseFor many dermatologists, physical abuse is rarely considered in the differential diagnosis of skin lesions, even though these are the most common sign of abuse (present in over 90% of cases) and are easily recognizable. One logical explanation might be that dermatologists have little or no training in this area. Distinguishing injuries caused by abuse from accidental injuries, benign skin conditions, or specific skin diseases in a child, can be difficult. It is essential to take a thorough history (with separate child and parent interviews) and to perform a full examination of the skin, appendages, and mucous membranes. The investigation should also include X-rays and, where appropriate, blood tests. Warning signs of abuse include a vague explanation by the caretakers of how the child's injuries occurred, conflicting versions by the parents, a story that changes over time, a history of frequent visits to the emergency room or of multiple fractures, and an unjustified delay in seeking medical care. A story that is inconsistent with the physical signs, or that is implausible considering the child's motor skills (for example when a child who is not old enough to crawl is reported to have fallen down the stairs), is highly suggestive of abuse.6 Cutaneous manifestations of abuse include bruising, contusions, erosions, lacerations, burns, bites, and traumatic alopecia.
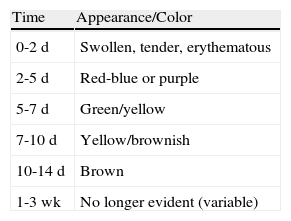
Bruising is the most common sign of physical abuse.7 Because bruises are common in any active child, the challenge lies in distinguishing those resulting from abuse from those caused accidentally. Accidental bruises tend to be found in bony prominences, above all on the knees, the shins, the elbows, and the forehead. Bruises found in soft or generally protected areas such as the buttocks, the back, the trunk, the arms, the genitalia, the inner thighs, the ears, the cheeks, and the neck may indicate abuse. In particular, bruising on the genitalia and ears are highly suspicious signs of abuse.8 Likewise, bruises and bumps should be treated with suspicion in children younger than 9 months as they are unable to move around.9 The type of bruise must also be examined carefully. Linear shapes, above all on the back and the buttocks, suggest injury by a rope, a belt, a cord, or a wire (Figs. 1-3). Fingertip bruises may be seen on the arms of a child who has been grabbed forcefully, while purple, finger-edge (linear) bruises are typically found on the cheeks of a child who has been slapped. Wraparound bruises or circumferential wounds or bruising on the wrists, ankles, neck, or at the corners of the mouth are virtually pathognomonic of physical abuse. The presence of bruises at different stages of healing is a sign that deserves special attention as it can help to distinguish between inflicted and accidental bruises. Dermatologists must also be familiar with how bruises change as they age. Both the color and shape of a bruise can provide clues as to when the injury occurred (Table 1). It is generally accepted that a bruise with a yellow color is at least 18hours old, although the absence of yellow does not mean that the injury occurred in the previous 18hours. Examination with a Wood lamp is useful for checking for faint and subclinical bruising.10 The characteristics of bruises, however, depend on a number of factors, including the age, location, and depth of the bruise, the child's age and skin type, the force of the injury that caused the bruise, and the presence of disease.11 Particular care should thus be taken when examining bruises.
.")
.")
.")
Human bite marks are also a clear sign of abuse and call for a full physical examination. A human bite should be suspected when ecchymoses or lacerations with an elliptical or ovoid shape are observed. Animal bites tend to be deeper and also generally cause more severe skin damage. The shape of the bite is clearest 2 to 3 days after the injury, when the swelling subsides and erythema appears around the wound. Adult bites can be easily distinguished from those caused by children by measuring intercanine distance. If the distance is greater than 3cm, it can generally be assumed that the bite was inflicted by an adult.12 Bite marks are of particular relevance because they have been associated, with relatively frequency, with sexual abuse.
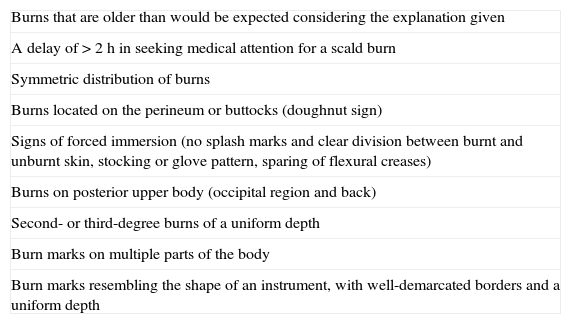
Burns account for between 6% and 20% of all child abuse injuries and it has been estimated that up to 25% of all burns in children are inflicted.13 Children under 3 years of age are the most affected, and tap water scalds are the most common type of burn observed. Accidental burns caused by the spattering of hot liquids or contact with hot objects are common in children, but there are characteristic features that are highly suggestive of abuse (Table 2). Children with a history of burn injuries or with bilateral, symmetric burns should be examined carefully, as should children in whom there was a delay of more than 2hours in seeking medical attention. It is also important to note that while a burn may have been accidental, it may have occurred due to a lack or supervision or neglect. Such cases also need to be reported.
Characteristics Suggestive of Inflicted Burns.
| Burns that are older than would be expected considering the explanation given |
| A delay of > 2 h in seeking medical attention for a scald burn |
| Symmetric distribution of burns |
| Burns located on the perineum or buttocks (doughnut sign) |
| Signs of forced immersion (no splash marks and clear division between burnt and unburnt skin, stocking or glove pattern, sparing of flexural creases) |
| Burns on posterior upper body (occipital region and back) |
| Second- or third-degree burns of a uniform depth |
| Burn marks on multiple parts of the body |
| Burn marks resembling the shape of an instrument, with well-demarcated borders and a uniform depth |
Stratman and Melski14 described 3 classic signs of forced immersion in hot water: stocking and glove burns, zebra stripe burns, and doughnut hole burns. Stocking and glove burns refer to deep, symmetric second- or third-degree burns on the hands or feet of a child, caused by prolonged immersion in a hot liquid. A doughnut hole burn may be observed on the buttocks of a child forced to sit in a hot bathtub (the hole corresponds to the skin that was spared from burning because it was in contact with the cooler surface of the bottom of the tub). Finally, zebra stripe burns are seen when a child's arms or legs are forcibly immersed in hot water in a flexed position. In this case, the flexural creases are spared from contact with the hot water. Contact burns, caused by forced contact with a hot object, tend to have the same shape as the object. Cigarette burns, for example, are characteristically third-degree burns with a diameter of 7 to 10mm; they generally have a punched-out appearance, heal slowly, and cause scarring. They tend to be found on the face, the palms, the soles and the genitalia (Figs. 4 and 5)15.
.")
.")
Alopecia, while less common, can also be a sign of physical abuse. Traumatic alopecia is characterized by areas of hair loss which are often ecchymotic and have highly irregular borders.16 This type of alopecia is generally painful and may be seen in association with subgaleal hemorrhage and a scalp surface with an abnormal contour (due to the presence of underlying hematomas).
Traumatic alopecia can be difficult to distinguish from similar, more common conditions, such as tinea capitis, traction alopecia, alopecia areata, loose anagen syndrome, and, in particular, trichotillomania. Children with trichotillomania, however, generally have hairs broken at more varying lengths than those who are victims of child abuse.
Differential DiagnosisDermatologists are responsible for distinguishing skin lesions caused by abuse from skin conditions, benign or otherwise, that can mimic abuse. The most common markings confused with bruises by physicians who are not dermatologists are Mongolian spots,17 which are frequently found on the buttocks and the back. Unlike bruises, however, these spots are not painful and their appearance does not change significantly over days or weeks.
A complete coagulation study should be ordered in children with multiple bruises to rule out an underlying blood disorder (mainly hemophilia, von Willebrand disease, idiopathic thrombocytopenic purpura, and vitamin K deficiency). Idiopathic thrombocytopenic purpura and leukemia must be considered in children with petechiae and multiple hematomas. Patients with coagulation factor deficiencies typically have deep circular bruises with indurated centers. When such a deficiency is suspected, it is essential to take a personal and family history of bruising and tendency to bleed.
Certain forms of vasculitis that typically present in childhood (eg, Schönlein-Henoch syndrome and acute hemorrhagic edema of infancy) can occasionally cause purple erythematous, edematous plaques that can mimic inflicted injuries. Children with Schönlein-Henoch syndrome often have lesions on the legs and buttocks, frequently in association with a previous infection and abdominal and joint pain.
Various conditions, including perniosis, erythema nodosum, and hemangiomas, have been confused with physical abuse. Blisters can also mimic burns in the following disorders: staphylococcal scalded skin syndrome, bullous impetigo, linear IgA dermatosis, and fixed drug eruption. Finally, infections such as erysipelas and ecthyma as well as certain forms of dermatitis (phytophotodermatitis, contact dermatitis, and diaper rash) should also be considered in the differential diagnosis of a child with burn-like marks.18
Physical NeglectPhysical neglect is more common than physical abuse and can also be diagnosed on the basis of skin findings. Physical neglect can be defined as a progressive deterioration in the physical state of a child or an adolescent due to failure or inability on the part of the parents or caretakers to provide the necessary care (food, clothing, hygiene, protection, and supervision), despite having the means to do so. A victim of physical neglect will generally have a combination of characteristics that should raise suspicion, for example, poor hygiene and inappropriate clothing, markedly decreased subcutaneous tissue due to malnutrition, severe dermatitis (particularly in the diaper area) (Fig. 6), and dry or scaly skin caused by nutritional deficiencies. Parasite infections (particularly lice infestation) are also common. Other signs of possible child neglect are unhealed injuries or an inexplicable delay in seeking medical care after an injury.
Sexual Abuse.")
Sexual abuse is unfortunately a common occurrence in children. It affects boys and girls of all ages, races, and socioeconomic backgrounds and can cause serious physical and psychological harm. Girls are at greatest risk, with risk increasing in preadolescence. Several studies have shown that between 12% and 25% of women and between 8% and 10% of men have experienced some form of sexual abuse during childhood or adolescence.19 Ninety percent of the perpetrators are men, who, in most cases (70%-90%), are relatives or acquaintances of the child. Because of its frequency, implications, and possible consequences, sexual abuse must be considered in the initial differential diagnosis of anogenital lesions in children and adolescents. To be able to make an early diagnosis, the dermatologist must be familiar with the cutaneous signs that are suggestive of sexual abuse.
It is important to note that sexual abuse is not limited to penetration. According to the current definition, it also includes inappropriate touching, caressing, and sexual kissing. Most children who are victims of sexual abuse do not have physical signs, and often, the only available evidence is the verbal account of the child. Studies have shown that, even in confirmed cases of sexual abuse, less than 5% of victims have suspicious findings on physical examination.20 It seems to have been demonstrated that the presence of anogenital lesions in sexual abuse is inversely correlated with the time between the event and the clinical visit (probably because the lesions heal rapidly) and that anogenital lesions are more likely to be present if the patient reports bleeding during the sexual act.
Dermatologists are rarely consulted for frank vaginal bleeding but direct examination of the hymen can reveal signs suggestive of sexual abuse. The interpretation of hymenal notches and clefts depends on their location and severity. Findings that are highly suggestive of sexual abuse are acute hymenal tears (partial or complete), ecchymosis, absence of hymenal tissue in a specific area, and recent scars in the posterior fourchette.
In patients with purulent or foul-smelling vaginal discharge, specimens should be collected for culture to rule out sexually transmitted infection. Nonspecific vulvovaginitis, which is common in prepubertal girls, is not considered a sexually transmitted disease, but genital infections not acquired in the peripartum period (trichomoniasis, herpes simplex virus type 2, gonorrhea, syphilis, and human immunodeficiency virus infection) are highly suggestive of sexual abuse. Human papillomavirus infection is of particular relevance. Numerous studies have shown that genital warts can be acquired in the perinatal period (from an infected mother), through nonsexual contact with infected caretakers, and through autoinoculation from warts on other parts of the body. While nonsexual transmission is the most common cause of genital warts in children under 3 years of age, the presence of warts in a child aged over 5 years is a strong indicator of sexual abuse.2 The case of children between 3 and 5 years of age is less clear. There is also some discussion about the value of anogenital molluscum contagiosum as an indicator of sexual abuse.21
Perianal lacerations extending to the anal sphincter and considerable anal dilatation in the knee-chest position without a justifiable reason (constipation, feces in the rectal ampulla, or a neurologic disorder) (Figs. 7 and 8) are also highly suggestive of sexual abuse. Although lesions in the anogenital region may be less specific for sexual abuse, a record should be made of any fissures detected, particularly if they are located away from the midline.
.")
.")
While it is important to be alert to suspicious anogenital lesions, it is also important to perform a correct differential diagnosis, with consideration of conditions including lichen sclerosus et atrophicus, localized vulvar pemphigoid, pinworm infection, scabies, inverse psoriasis, atopic and contact dermatitis, perianal streptococcal dermatitis, and candidiasis.
When sexual abuse is suspected, it is also necessary to check for lesions in the mouth, although we believe that tests for traces of semen in the mouth and on other parts of the body using a Wood lamp is the responsibility of a forensic doctor. Pregnancy in a teenager might be an indication of sexual abuse in certain circumstances.
To conclude, we would like to highlight the important role of dermatologists in evaluating cutaneous signs suggestive of sexual abuse. Dermatologists need to be made aware of and encouraged to include child abuse in the differential diagnosis of any suspicious signs or symptoms. They also need to be encouraged to report all suspected cases to the relevant authorities. Sexual abuse should be considered whenever suspicious lesions are detected. These include multiple lesions at different stages of healing, lesions located in areas other than over bony prominences or in areas generally protected by clothing, lesions with an unusual shape, well-demarcated lesions surrounded by healthy skin, and lesions with a pattern suggesting injury by a specific instrument.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
We thank Dr Jordi Pou from Hospital Sant Joan de Déu in Barcelona, Spain, for kindly supplying the photographs used in this article.
Please cite this article as: Pau-Charles I, et al. Signos cutáneos del maltrato infantil. Actas Dermosifiliogr.2012;103:94-99.



