








A large number of flaps, particularly rotation and transposition flaps, have been described for the closure of skin defects left by oncologic surgery of the nose. The logarithmic spiral flap is a variant of the rotation flap.
Materials and methodsWe present a series of 15 patients with different types of skin tumor on the nose. The skin defect resulting from excision of the tumor by micrographic surgery was reconstructed using various forms of the logarithmic spiral flap. There are 3 essential aspects to flap design: commencement of the pedicle at the upper or lower border of the wound, a width of the distal end of the flap equal to the vertical diameter of the defect, and a progressive increase in the radius of the spiral from the distal end of the flap to its base.
ResultsThe cosmetic and functional results of surgical reconstruction were satisfactory, and no patient required additional treatment to improve scar appearance.
ConclusionThe logarithmic spiral flap is useful for the closure of circular or oval defects situated on the lateral surface of the nose and nasal ala. The flap initiates at one of the borders of the wound as a pedicle with a radius that increases progressively to create a spiral. We propose the logarithmic spiral flap as an excellent option for the closure of circular or oval defects of the nose.
Para cerrar defectos cutáneos secundarios a cirugía oncológica en la pirámide nasal se han descrito un elevado número de colgajos, entre los que destacan los de rotación y transposición. El colgajo en espiral logarítmica se considera una variante del colgajo de rotación.
Materiales y métodosPresentamos una serie de 15 pacientes con diferentes tipos de neoplasias cutáneas en la pirámide nasal en los que el defecto cutáneo tras la exéresis mediante cirugía controlada al microscopio fue reconstruido mediante diferentes opciones de colgajo en espiral logarítmica. En el diseño del colgajo existen 3 aspectos esenciales: iniciar el pedículo en el borde superior o inferior de la herida, procurar que la anchura del extremo distal sea equivalente al diámetro vertical del defecto y aumentar progresivamente el radio desde el extremo distal del colgajo hasta su base.
ResultadosLos resultados estético y funcional tras la reconstrucción quirúrgica fueron adecuados, y ningún paciente requirió tratamientos adicionales para mejorar el aspecto de la cicatriz.
ConclusiónEl colgajo en espiral logarítmica es útil en el cierre de defectos con morfología circular u ovalada localizados en el ala y lateral nasal, y se diseña desde uno de los bordes de la herida como un pedículo que, a modo de espiral, va aumentando progresivamente su radio. Proponemos el colgajo en espiral logarítmica como una opción excelente por un buen resultado estético en el cierre de defectos circulares u ovalados de la pirámide nasal.
There are a number of surgical options for the reconstruction of small circular or oval defects on the external nose. The most relevant are healing by second intention, primary closure, partial or full-thickness skin grafts, lobed and geometric transposition flaps, and rotation flaps. The rotation flaps include a type called the spiral flap.
The logarithmic spiral flap is designed starting at one of the borders of the wound as a pedicle whose radius progressively increases in the form of a spiral.
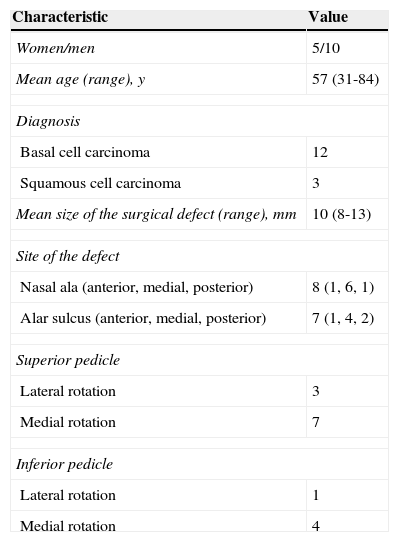
Material and MethodsWe present a series of 15 patients who underwent excision of different types of skin tumor on the external nose using micrographic surgery between January 2011 and January 2015 (Table 1). The resulting skin defects were reconstructed using logarithmic spiral flaps. The patients were 5 women and 10 men, with a mean age of 57 years.
Patient Characteristics.
| Characteristic | Value |
|---|---|
| Women/men | 5/10 |
| Mean age (range), y | 57 (31-84) |
| Diagnosis | |
| Basal cell carcinoma | 12 |
| Squamous cell carcinoma | 3 |
| Mean size of the surgical defect (range), mm | 10 (8-13) |
| Site of the defect | |
| Nasal ala (anterior, medial, posterior) | 8 (1, 6, 1) |
| Alar sulcus (anterior, medial, posterior) | 7 (1, 4, 2) |
| Superior pedicle | |
| Lateral rotation | 3 |
| Medial rotation | 7 |
| Inferior pedicle | |
| Lateral rotation | 1 |
| Medial rotation | 4 |
The most important aspect is a correct design of the flap, which must extend along approximately half of the perimeter of a theoretical circumference. The pedicle can be superior or inferior, and each one of the these can, in turn, use medial rotation (parallel to the dorsum of the nose) or lateral rotation (perpendicular to the dorsum of the nose) (Fig. 1).

For circular defects, the first step is to draw the vertical and horizontal axes of the defect, which will have the same length (X). The tangent of the superior border of the defect is then drawn parallel to the horizontal axis, and the vertical axis is extended superiorly or inferiorly, depending on the design of the pedicle. Three points are required to design the spiral: the first is the point of intersection between the vertical axis and the inferior border of the defect; the second is the point on the tangent at a distance of 1.15X from the vertical axis; the third is the point on the prolongation of the vertical axis, situated at 1.3X from the superior border of the defect (Figs. 2 and 3).
. B, The tangent is drawn across the superior border of the defect, parallel to the horizontal axis; the vertical axis of the defect is extended. C, The point of intersection between the vertical axis and the inferior border of the defect is marked. D, The second point is situated on the tangent at a distance of 1.15X from the vertical axis. E, The third point of intersection is marked on the prolongation of the vertical axis, at a distance of 1.3X from the superior border of the defect. F, The logarithmic spiral is designed using these 3 points.")
A, The vertical and horizontal axes of the defect are drawn; these axes are of the same length (X). B, The tangent is drawn across the superior border of the defect, parallel to the horizontal axis; the vertical axis of the defect is extended. C, The point of intersection between the vertical axis and the inferior border of the defect is marked. D, The second point is situated on the tangent at a distance of 1.15X from the vertical axis. E, The third point of intersection is marked on the prolongation of the vertical axis, at a distance of 1.3X from the superior border of the defect. F, The logarithmic spiral is designed using these 3 points.

After drawing the design, the flap is dissected in the subcutaneous plane, and the distal end is rotated on itself to cover the defect. A subcutaneous stitch of 4/0 or 5/0 polyglycolic acid (Dexon) is placed to attach the proximal part of the pedicle to the middle of the semicircle of the design. No sutures should be placed at the tip of the flap as this could compromise the blood supply. A 6/0 silk suture is then used to close the remaining defect, displacing the flap to adapt it to the peri-incisional skin (Figs. 4–8).
 and 6/0 silk. A small concave area was left open. This healed correctly within a few days by second intention. E, Result at 24hours. F, Appearance at 6 months.")
A, Basal cell carcinoma on the left nasal ala. B, Design of a logarithmic spiral flap with a superior pedicle. C, Flap dissected in the subcutaneous plane. D, After medial rotation of the flap, it was sutured using a 4/0 polyglycolic acid suture (Dexon) and 6/0 silk. A small concave area was left open. This healed correctly within a few days by second intention. E, Result at 24hours. F, Appearance at 6 months.
 and 6/0 silk. F, Result at 24hours.")
A, Basal cell carcinoma on the lateral surface of the nose. B, Logarithmic spiral flap with a superior pedicle. C, An oval defect was left on the nasal ala. D, The flap was dissected in a deep plane. E, Medial rotation of the flap, parallel to the dorsum of the nose, and suture with a 4/0 polyglycolic acid suture (Dexon) and 6/0 silk. F, Result at 24hours.

 and 6/0 silk. E, Result at 24hours. F, Appearance at 2 months.")

The cosmetic result after surgical reconstruction was adequate, and none of the patients required additional treatment to improve the appearance of the scar. Respiratory function was preserved in all cases (Figs. 4–8). The main limitation observed was a minimal retraction of the nasal ala after surgery in 1 patient; this occurred because the pedicle was initiated on the medial border of the defect rather than on its inferior or superior border. In some patients a small central area was left open at the point of maximum tension to avoid vascular compromise of the displaced tissue. These areas healed correctly and spontaneously within a few days (Figs. 4 and 5).
DiscussionPrimary vertical closure is an appropriate option for the reconstruction of small defects of the nasal ala; however, this is not possible for larger lesions because of the high likelihood of subsequent asymmetry due to traction on the ala. Although second-intention healing produces acceptable results in concave areas of the external nose, hypertrophic scars can develop in convex areas, with traction on the ala giving rise to asymmetry.1 Pipitone and Gloster2 proposed a combination of partial primary closure and healing by second intention as an option for the reconstruction of defects of the nasal ala.
The cosmetic results of skin grafts to the nasal ala are usually poorer, with healing defects or persistent edema. In a series of 168 patients with small defects on the nasal ala that were reconstructed with full-thickness skin grafts, 93 required an intervention to improve the cosmetic appearance: 67 by triamcinolone acetonide injection, 14 by a combination of triamcinolone injections and laser, and 12 by laser alone.3
The Limberg and Dufourmentel transposition flap is useful to cover geometric rhomboid defects, but it is not so effective in round or oval defects.4 Digitiform and lobed flaps that transpose adjacent skin frequently produce lumps, with a very unsightly trap-door effect.
The spiral flap is a modification of the rotation flap and achieves better functional and cosmetic results. Humphreys5 proposed the reconstruction of small defects of the nasal ala using a spiral flap in which the incision was made along the nasal sulcus. In some patients in that study, their technique gave rise to retraction and asymmetry of the ala that required triamcinolone injections in the postoperative period for correction. Stoner and Stoner6 described another variant of the spiral flap in which the risk of retraction was reduced by making the incision along one of the borders of the ala, thus taking advantage of the surrounding skin to increase freedom of movement during reconstruction of the defect. However, the total length of the incision sometimes had to be longer, reaching the nasolabial fold, which increased the risk of traction on the ala and an unacceptable cosmetic result.
We present a series of patients with nasal defects reconstructed using spiral flaps for which, as in the report by Stoner and Stoner,6 the incision was made along one of the borders of the nasal ala. However, in contrast to those authors, we used the technique described by Mahlberg et al.,7 in which the flap had a logarithmic design that produced a spiral with a diameter that progressively increased along the length of the flap rather than remaining constant. This increases the surface area of the flap and creates a larger vascular pedicle, reducing the risk of necrosis.
Although there are 4 options for the logarithmic spiral flap, the use of an inferior pedicle is much more limited than a superior pedicle, as it is only indicated for defects high up on the nose, at a distance from the nasal ala. Also, depending on the size and design, an inferior pedicle can give rise to traction on the ala and produce asymmetry.
During reconstruction using a logarithmic spiral flap, the most important factor is the initial design, which consists of drawing the point of intersection between the vertical axis (X) and the inferior border of the defect, another point of intersection on the tangent of the superior border, situated at a distance of 1.15X from the vertical axis, and a third point on the prolongation of the vertical axis, at a distance of 1.3X from the superior border of the defect. These 3 points will guide the design of the logarithmic spiral, as they ensure a progressive increase in the radius from the distal end of the flap to its base.
Likewise, it should be noted that, depending on the size and site of the defect, as well as on the nasal physionomy of each patient, the design cannot always be initiated at the superior or inferior border of the defect, but rather it must occasionally be more medial or lateral; in all cases, the flap must occupy half the perimeter of a theoretical circumference (Figs. 2 and 3).
The matter of leaving a minimal area unsutured, coinciding with the concave area of the center of the defect, is not a problem, as this will heal correctly by second intention.
In summary, we have proposed the logarithmic spiral flap as a very useful, cosmetically acceptable, and functional alternative for the closure of circular or oval defects on the external nose.
Ethical disclosuresProtection of human and animal subjects.The authors declare that no experiments were performed on humans or animals for this research.
Confidentiality of dataThe authors declare that no private patient data are disclosed in this article.
Right to privacy and informed consentThe authors obtained informed consent from the patients and/or subjects referred to in this article. This document is held by the corresponding author.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Moreno-Artero E, Redondo P. Colgajo en espiral logarítmica para defectos circulares u ovalados en superficie lateral y ala nasal. Una serie de 15 casos. Actas Dermosifiliogr. 2015;106:658–665.


