

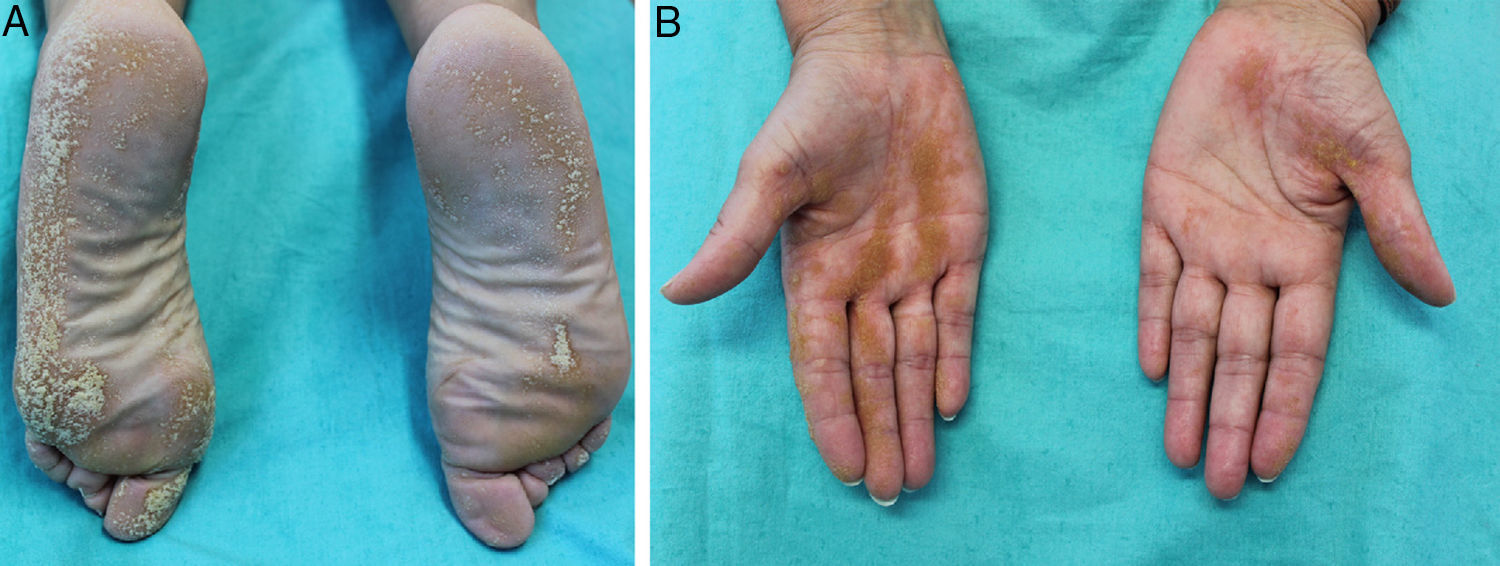
A 42-year-old woman with no personal or family history of interest presented with asymptomatic cutaneous lesions that has been on her palms and soles for 20 years (Fig. 1). She had been diagnosed with psoriasis at another hospital but had shown no improvement with corticosteroids. Physical examination revealed multiple yellowish-whitish hyperkeratotic papules that converged to form linear wart-like plaques and punctate pits with keratotic plugs on the palms, soles, and digits. Biopsy showed epidermal invagination with a column of parakeratotic cells with an absent granular layer and dyskeratotic cells in the underlying eccrine duct. The patient was diagnosed with porokeratotic eccrine ostial and dermal duct nevus (PEODDN).
The etiology of PEODDN is unknown, but findings point to a possible genetic mosaicism that causes abnormal keratinizing epidermal invagination traversed by an acrosyringium. The condition can appear at birth, in childhood, or in adulthood. It mainly affects the palms and soles and may be accompanied by pruritus, hyperhidrosis, or anhidrosis. The differential diagnosis should include blaschkoid porokeratotic and linear verrucous epidermal nevus, linear porokeratosis, linear psoriasis, punctate keratoderma, and nevus comedonicus. Diagnosis must be confirmed histologically. Lesions can resolve spontaneously or persist. Treatments include carbon dioxide laser therapy, keratolytics, retinoids, corticosteroids, calcipotriol, anthralin, phototherapy, cryotherapy, and electrosurgery.
Please cite this article as: Imbernón-Moya A, Aguilar-Martínez A, Vargas-Laguna E. Queratodermia palmoplantar lineal. Actas Dermosifiliogr. 2018;109:269.



