




The patient was a 16-year-old girl with a past history of cholangitis, reactive arthritis, and stable plaque morphea who had been receiving follow-up rheumatologic and dermatologic care. During a routine follow-up visit, the patient reported the appearance of asymptomatic plaques on both cheeks that were mildly erythematous and rough to the touch.
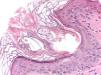
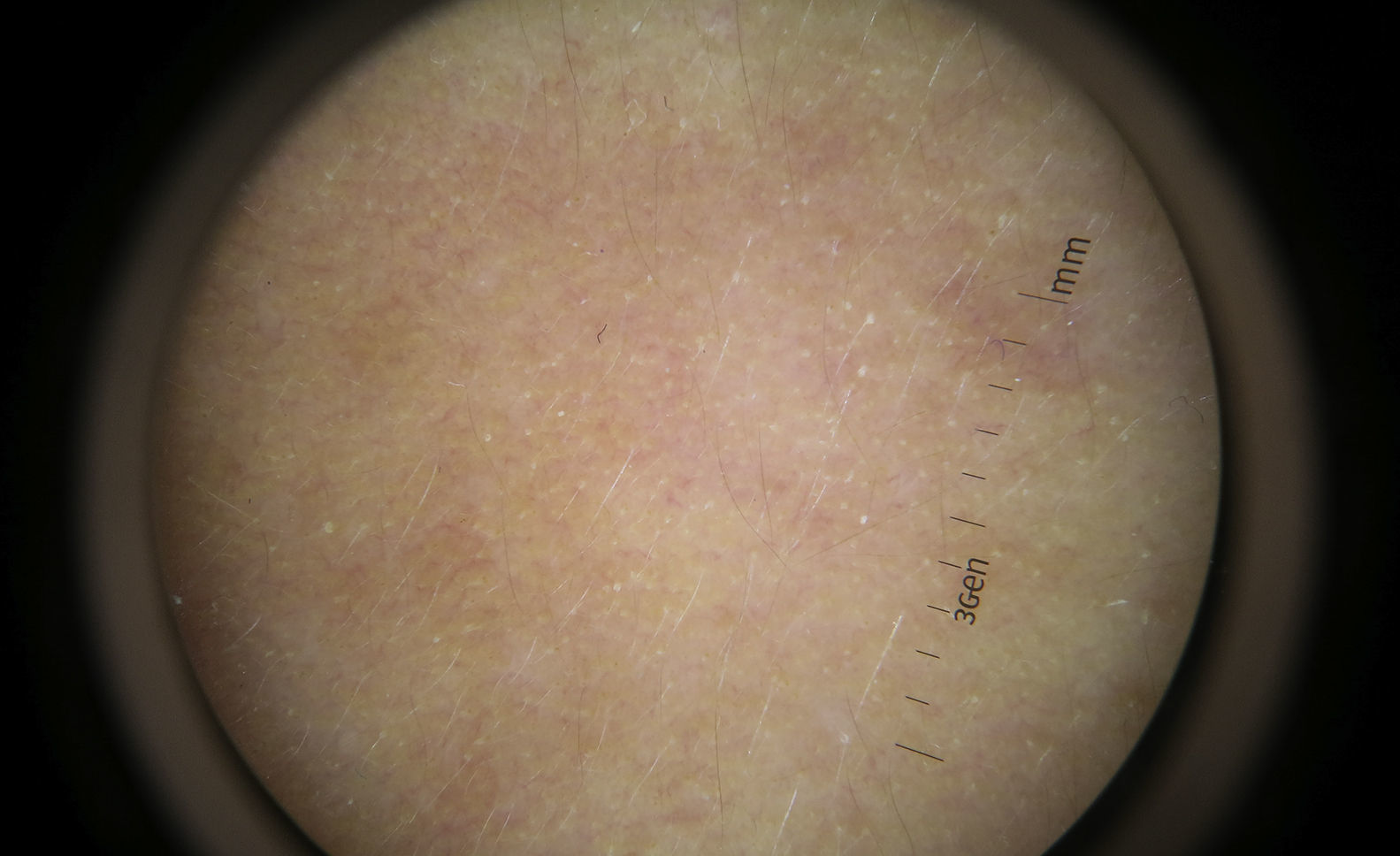
Physical ExaminationPhysical examination revealed facial skin with a xerotic appearance on both cheeks and along the mandibular rami and erythematous plaques with a distinct border (Fig. 1). Dermoscopy revealed hyperkeratosis and dilation of hair follicles (Fig. 2). On palpation, the skin had a rough, sandpaper-like texture. The skin examination was otherwise unremarkable.
Additional Tests
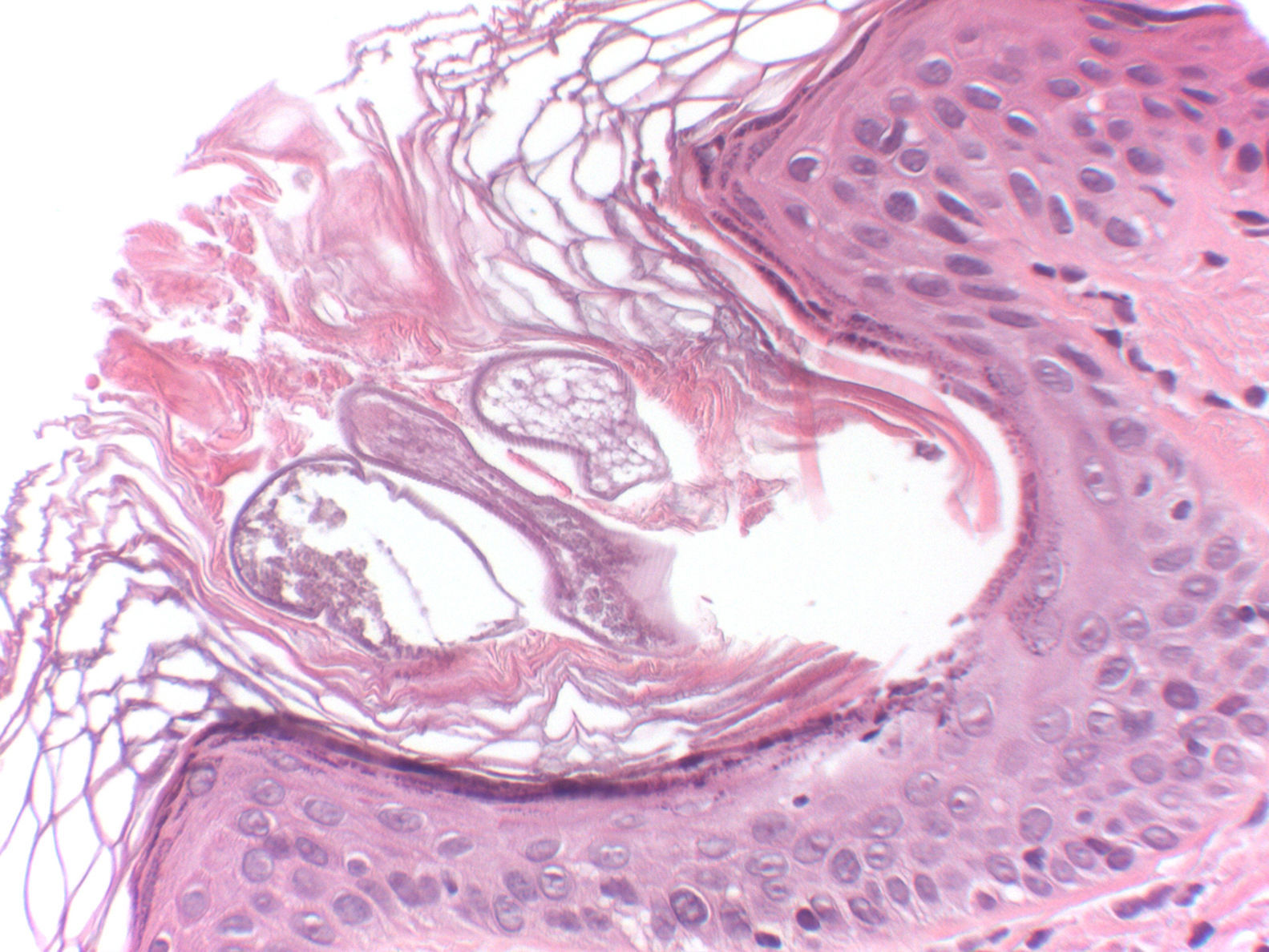
A 2-mm punch biopsy was taken from the left preauricular region. Histologic examination revealed the presence of 2 dilated follicular infundibula, with foci of compact hyperkeratosis, associated in both cases with the presence of a mite (Fig. 3). A mild perivascular lymphocytic inflammatory infiltrate was observed in the underlying dermis.
The complete blood count and biochemistry profile showed no abnormalities.
What Is Your Diagnosis?
DiagnosisSpinulosis of the face.
Clinical CourseFollowing histologic confirmation of spinulosis of the face associated with Demodex folliculorum, treatment was initiated with 0.5% ivermectin in carbohydrate-based cream once daily for 2 months. Clinical improvement was evident after 1 month of treatment and all signs had resolved by the end of treatment. No similar lesions have appeared during 6 months of follow-up.
CommentSpinulosis of the face is characterized by the presence of asymptomatic, hyperkeratotic, filiform spicules with a follicular distribution, located predominantly on the facial skin (cheeks, forehead, and chin). Although the association of this entity with D folliculorum was initially controversial, today the causal relationship is accepted.1,2
D folliculorum is a mite that is occasionally found in human skin in association with the pilosebaceous unit. This colonization is generally asymptomatic, but in predisposed individuals the presence of D folliculorum has been associated with various dermatoses, including rosacea, perioral dermatitis, and madarosis. The presence of 5 or more mites per square centimeter of skin or the presence of the mite in the dermis has been proposed as a pathogenic criterion.1,3
In the case of spinulosis of the face associated with D folliculorum, case series in patients with other diseases—particularly multiple myeloma and polycythemia vera—have been reported. Other associations with spinulosis of the face caused by D folliculorum include chronic renal failure, inflammatory bowel disease, and monoclonal gammopathy.1,4 Differential diagnosis should include eczema, seborrheic dermatitis, pityriasis folliculorum (which is also caused by D folliculorum but is associated with diffuse scaling, pruritus, and erythema, and in many cases with poor facial hygiene),4 and trichodysplasia spinulosa, a polyomavirus infection that occurs in immunocompromised patients and is characterized by hyperkeratotic spicules, especially on the face (nose, eyebrows, etc.), and causes the facial deformity leonine facies.5
Diagnosis is based on clinical suspicion. Thin spicules confined to the dilated follicular orifices of the face, making the skin of the affected areas rough to the touch, are highly characteristic. Histologic examination confirms the presence of the mite and hyperkeratotic material forming spicules in the follicular orifices.2 Like other skin diseases caused by Demodex mites, spinulosis of the face is treated with various specific antiparasitic agents. Topical treatment is sufficient in most cases. Drugs used include 0.75% metronidazole, 5% permethrin, and 0.5% ivermectin, with the latter achieving good response, as in our patient.6 In resistant cases, oral therapy with ivermectin or retinoids, among other drugs, can be used.1,3
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Ruiz-Rivero J, Domíngez MC, Blanco VP, Suárez-Fernández R. Hiperqueratosis folicular filiforme en la cara. Actas Dermosifiliogr. 2017;108:773–774.


