



The diagnosis of pigmented actinic keratosis can be complicated in clinical practice. The differential diagnosis with lentigo maligna melanoma can be difficult due to common clinical and dermoscopic characteristics. We present 5 cases of pigmented actinic keratosis in 4 patients. The most common dermoscopic finding was a grayish-brown granulation with a perifollicular distribution, present in all lesions, followed by rhomboidal structures in 4 cases, and an annular-granular pattern in 3. In no case were asymmetrical pigmented follicular openings observed. We draw attention to key findings that aid preoperative diagnosis of pigmented actinic keratosis.
El diagnóstico de las queratosis actínicas pigmentadas puede resultar complicado en la práctica clínica. El diagnóstico diferencial con el lentigo maligno melanoma plantea dificultades, tanto clínica como dermatoscópicamente, ya que ambas entidades pueden presentar características en común. Presentamos 5 casos de queratosis actínicas pigmentadas en 4 pacientes. El hallazgo dermatoscópico más frecuente fue una granulación marrón-grisácea de distribución perifolicular presente en todas las lesiones, seguido de estructuras romboidales en 4 y un patrón anular-granular en 3. En ningún caso se apreciaron salidas foliculares asimétricamente pigmentadas. Destacamos algunas claves que facilitan el diagnóstico preoperatorio de las queratosis actínicas pigmentadas.
Actinic keratosis is considered to be an in situ epidermal dysplasia that develops in sun-exposed areas in individuals with a fair skin phototype. In its pigmented forms it can be difficult to differentiate from lentigo maligna melanoma as the clinical features may be similar. As there is a marked difference in the prognosis and treatment of the 2 conditions, it would be very helpful if we could improve the accuracy of clinical diagnosis. Although the definitive diagnosis of skin tumors can only be established by histology, dermoscopy is a very useful tool that aids clinical diagnosis.1 We describe the clinical, dermoscopic, and histological features of 5 pigmented actinic keratoses in 4 patients and compare our findings with those reported in the literature.
Case DescriptionsThe 4 patients, 2 men and 2 women aged between 64 and 82 years, had pigmented facial lesions that had appeared 1 to 2 years earlier. Three patients had 1 lesion and 1 patient had 2 lesions. The clinical features are described in Table 1. The most common dermoscopic finding, present in all the lesions, was a grayish-brown perifollicular granulation; this was followed by rhomboidal structures (present in 4 lesions) and an annular-granular pattern (present in 3 lesions). Asymmetrically pigmented follicular openings were not observed in any of the lesions. Histology revealed a loss of the normal stratification of the epidermis, with atypical, melanin-laden keratinocytes in the basal layers. An inflammatory infiltrate of lymphocytes, histiocytes, and melanophages was observed in the dermis (Figs. 1–3).
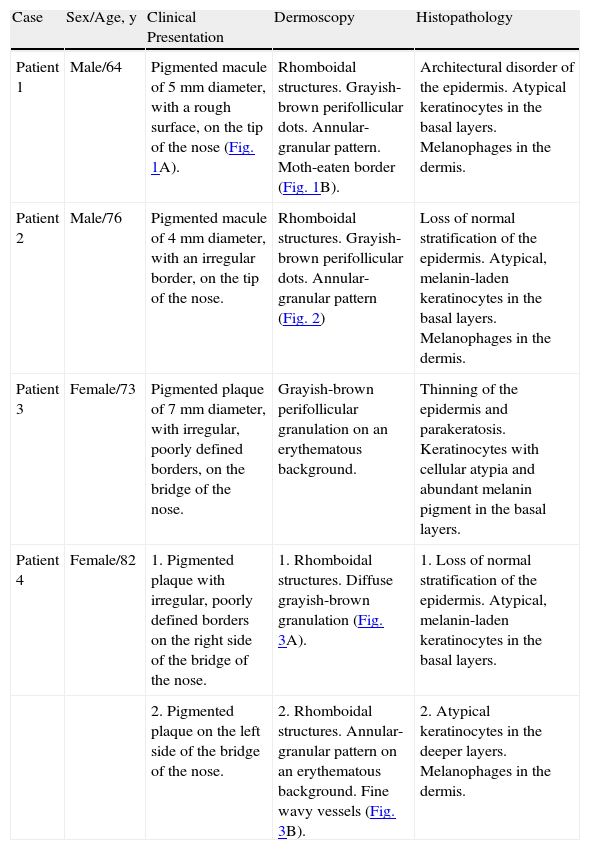
Epidemiological, Clinical, Dermoscopic, and Histological Features of Pigmented Actinic Keratosis.
| Case | Sex/Age, y | Clinical Presentation | Dermoscopy | Histopathology |
| Patient 1 | Male/64 | Pigmented macule of 5mm diameter, with a rough surface, on the tip of the nose (Fig. 1A). | Rhomboidal structures. Grayish-brown perifollicular dots. Annular-granular pattern. Moth-eaten border (Fig. 1B). | Architectural disorder of the epidermis. Atypical keratinocytes in the basal layers. Melanophages in the dermis. |
| Patient 2 | Male/76 | Pigmented macule of 4mm diameter, with an irregular border, on the tip of the nose. | Rhomboidal structures. Grayish-brown perifollicular dots. Annular-granular pattern (Fig. 2) | Loss of normal stratification of the epidermis. Atypical, melanin-laden keratinocytes in the basal layers. Melanophages in the dermis. |
| Patient 3 | Female/73 | Pigmented plaque of 7mm diameter, with irregular, poorly defined borders, on the bridge of the nose. | Grayish-brown perifollicular granulation on an erythematous background. | Thinning of the epidermis and parakeratosis. Keratinocytes with cellular atypia and abundant melanin pigment in the basal layers. |
| Patient 4 | Female/82 | 1. Pigmented plaque with irregular, poorly defined borders on the right side of the bridge of the nose. | 1. Rhomboidal structures. Diffuse grayish-brown granulation (Fig. 3A). | 1. Loss of normal stratification of the epidermis. Atypical, melanin-laden keratinocytes in the basal layers. |
| 2. Pigmented plaque on the left side of the bridge of the nose. | 2. Rhomboidal structures. Annular-granular pattern on an erythematous background. Fine wavy vessels (Fig. 3B). | 2. Atypical keratinocytes in the deeper layers. Melanophages in the dermis. |

A, Clinical image of the lesion in patient 1. There is a dark brown, pigmented macule of 5mm diameter, with well-defined borders and a slightly rough surface. Part of the border of the lesion is moth-eaten. B, Dermoscopic image of the lesion in patient 1, showing rhomboidal structures and an annular-granular pattern.


A, Dermoscopic image of the lesion on the right side of the bridge of the nose in patient 4. Rhomboidal structures can be seen on an erythematous background and there is a diffuse grayish-brown granulation. B, Dermoscopic image of the lesion on the left side of the bridge of the nose, showing rhomboidal structures and an annular-granular pattern in the inferior part of the lesion. The same structures were observed in the superior part of the lesion, but with a more reddish color and with a number of fine wavy vessels.
The pigmented forms of actinic keratosis are relatively rare variants that can present similar clinical features to malignant lesions, such as melanoma, or benign lesions, such as senile lentigo or seborrheic keratosis.2,3
Dermoscopy has been shown to improve accuracy in the diagnosis of pigmented lesions, particularly melanoma.4 Pigmented lesions on the face are characterized by the presence of a pigmented pseudonetwork caused by a lower density of rete ridges and a higher density of adnexal structures in this region.5 These characteristics of the facial skin mean that the criteria applied to pigmented facial lesions are different from those used for other areas of the body.
There are many publications that describe the dermoscopic features of facial melanoma and their histological correlations.6,7 According to the model for melanoma progression, asymmetrically pigmented follicular openings, rhomboidal structures, and an annular-granular pattern are the most frequently observed dermoscopic findings.6 However, there are few studies on the use of dermoscopy in pigmented actinic keratosis.1,2,8 A pigmented pseudonetwork of grayish-brown color has been reported in some lesions; this corresponds histologically with hyperpigmentation of the Malpighian layer interrupted by the follicular openings. Other studies describe multiple grayish-brown dots and globules around the hair follicles2; this finding was present in all the actinic keratoses in our series. The coalescence of these dots and globules, which have been shown histologically to be due to the presence of aggregates of melanin and macrophages in the papillary dermis, produces the annular-granular pattern. Another feature, the moth-eaten border typical of senile lentigo and seborrheic keratosis, has also been described in pigmented actinic keratosis1 and was observed in 1 of the lesions in this study.
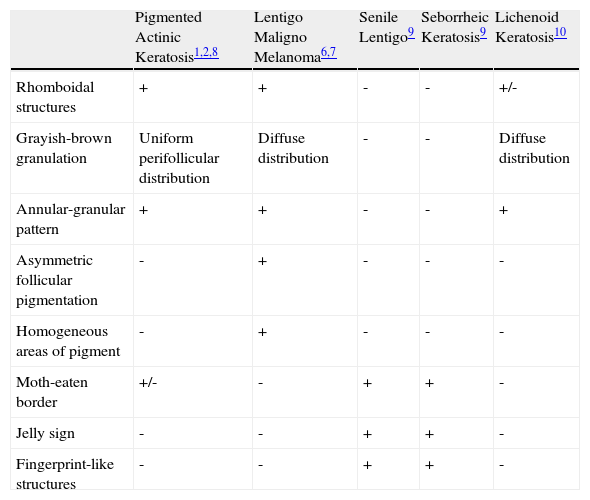
The principal differential diagnosis of pigmented actinic keratosis is with lentigo maligna, though senile lentigo, seborrheic keratosis, and lichenoid keratosis should also be considered. Dermoscopy can reveal certain details that help to differentiate between these conditions (Table 2). Asymmetrically pigmented follicular openings can be seen in the early stages of lentigo maligna, but they have not been observed in pigmented actinic keratosis and were not seen in any of the lesions in our series. This sign indicates invasion of the hair follicles by malignant melanocytes.1,9 In addition, the perifollicular dots and globules of lentigo maligna are less regular in diameter, color, and distribution than those observed in pigmented actinic keratosis.2 Another finding in favor of a diagnosis of melanoma is the presence of a hyperpigmented ring around the follicular openings, a sign not reported in pigmented actinic keratosis.6,9
Dermoscopic Differential Diagnosis of Pigmented Facial Lesions.
| Pigmented Actinic Keratosis1,2,8 | Lentigo Maligno Melanoma6,7 | Senile Lentigo9 | Seborrheic Keratosis9 | Lichenoid Keratosis10 | |
| Rhomboidal structures | + | + | - | - | +/- |
| Grayish-brown granulation | Uniform perifollicular distribution | Diffuse distribution | - | - | Diffuse distribution |
| Annular-granular pattern | + | + | - | - | + |
| Asymmetric follicular pigmentation | - | + | - | - | - |
| Homogeneous areas of pigment | - | + | - | - | - |
| Moth-eaten border | +/- | - | + | + | - |
| Jelly sign | - | - | + | + | - |
| Fingerprint-like structures | - | - | + | + | - |
Grayish-brown perifollicular granules were observed in all the lesions in our series. The granules were homogeneous in color and diameter and tended to occur in an ordered and uniform annular-granular pattern. We did not observe any asymmetrically pigmented follicular openings or homogeneous areas of pigmentation. Rhomboidal structures were a common finding in our patients. These patterns coincide with those reported in previous studies and may be defined as typical dermoscopic features of pigmented actinic keratosis.
In conclusion, the main value of dermoscopy in pigmented actinic keratosis is in the differential diagnosis with lentigo maligna, particularly in complex cases in which the clinical presentation is ambiguous. A single dermoscopic criterion may be insufficient, but the correlation between the clinical presentation of the lesion and the dermoscopic patterns observed could improve the accuracy of the noninvasive diagnosis of pigmented facial lesions.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Ciudad C, et al. Utilidad de la dermatoscopia en el diagnóstico de las queratosis actínicas pigmentadas. Actas Dermosifiliogr.2011;102:623-6.



