



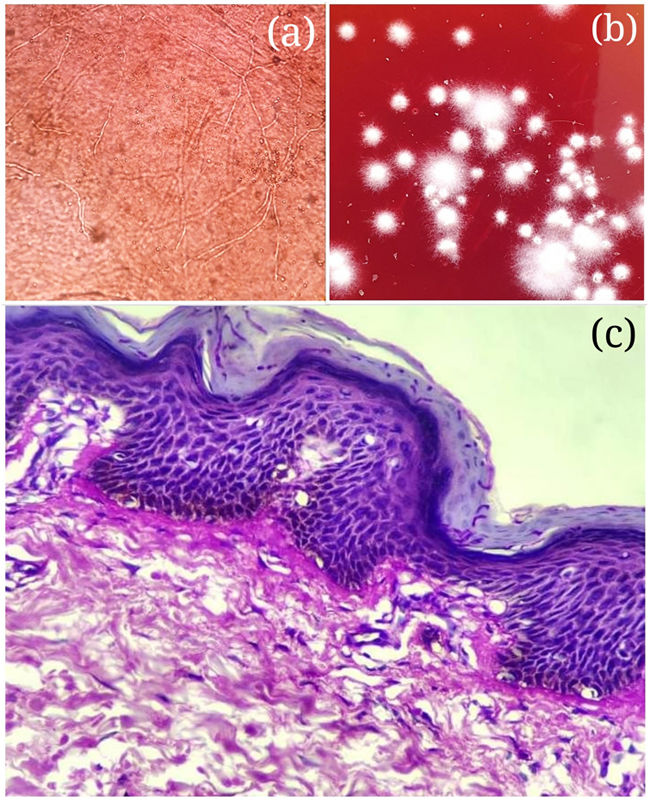
A 40-year-old female came with itchy, large plaque with silvery scales covering anterior trunk, groin (Fig. 1a) and buttocks since 8 months. There was no central clearing. The patient used non prescriptional topical preparation containing mixtures of Clobetasol propionate 0.05%, and Clotrimazol 1%. Laboratory investigations including complete blood count, blood sugar level, thyroid, renal and liver function tests were within normal limits. Test for HIV was negative. We kept differential diagnosis as psoriasis vulgaris, mycosis fungoides and psoriasiform dermatophytosis. Potassium hydroxide mount demonstrated septate fungal hyphe (Fig. 2a). Fungal culture showed white cottony colonies of T. Rubrum on Sabouraude's agar (Fig. 2b). Histopathology showed focal parakeratosis, focal spongiosis, with fungal hyphe in hyperplastic epidermis. PAS stain confirmed dermatophytosis (Fig. 2c).

Itraconazole 100mg twice daily along with Sertaconazole 1% cream and levocetrizine 5mg showed good improvement after one month (Fig. 1b). It was continued for further 2 months till complete recovery.
Psoriasiform dermatoses constitute disorders which clinically and/or histologically resemble psoriasis. Atypical lesions of tinea can be seen in both immune-competent and immune-compromised patients. Immunosuppressant effect of topical corticosteroids can lead to reduced local inflammation which allows slow growth of fungus and less erythema or scaling giving psoriasis like appearance.
Unscrupulous self medication of potent topical creams for dermatophytosis is dangerous and often results into highly infectious chronic progressive and treatment resistant tinea infection.



