
Phototherapy involves the use of UV radiation to treat different dermatologic diseases. Its efficacy and safety have been thoroughly established in adults and some publications indicate that it is also an effective and safe treatment in pediatric patients with refractory skin diseases.
Material and methodsRetrospective study that included all patients under 17 years of age and 122 randomly selected adults who received phototherapy in our department between 2002 and 2017.
ResultsNinety-eight pediatric patients (61% girls and 39% boys) with a mean age of 10.5 years received phototherapy. The 3 most frequently treated diseases were psoriasis (48% of patients), vitiligo (17%), and atopic dermatitis (16%). Eighty-six percent of the patients received phototherapy with narrowband UV-B, whereas 7% received phototherapy with psoralen and UV-A (PUVA). No statistically significant differences were found in terms of dosage, duration, or number of sessions compared to the adult population treated with narrowband UV-B therapy or PUVA. A complete response was achieved in 35% of the pediatric patients and no differences were found with respect to the adults. Only 16% of the children showed adverse effects, mostly in the form of mild erythema. We found greater adherence to treatment in the pediatric patients than in the adult patients (P <.05).
ConclusionsNarrowband UV-B therapy and PUVA appear to be safe and effective in children and can be administered using the same treatment protocols as those used in adults. Adherence to treatment is greater in children than in adult patients.
la fototerapia se basa en el uso de radiación ultravioleta para el tratamiento de distintas patologías dermatológicas. Su eficacia y seguridad está ampliamente establecida en adultos y existen publicaciones que también lo avalan como un tratamiento efectivo y seguro en pacientes pediátricos con afecciones cutáneas recalcitrantes.
Material y métodosestudio retrospectivo desde 2002 hasta 2017 que incluye a todos los pacientes menores de 17 años que recibieron fototerapia en nuestro servicio. Además, se seleccionaron al azar 122 pacientes adultos que recibieron este tratamiento durante el mismo periodo de tiempo.
Resultadosse realizaron un total de 98 tratamientos pediátricos, 61% en niñas y 39% en niños, con una media de edad de 10,5 años. Las 3 patologías más frecuentemente tratadas fueron la psoriasis (48% de pacientes), el vitíligo (17%) y la dermatitis atópica (16%). El 86% de los pacientes recibieron fototerapia con radiación ultravioleta B de banda estrecha (UVB-BE), mientras que el 7% recibieron fototerapia con radiación ultravioleta A con psoralenos (PUVA). No existían diferencias estadísticamente significativas en cuanto a dosis, duración o número de sesiones con respecto a la población adulta tratada con UVB-BE ni con PUVA. Se alcanzó una respuesta completa en el 35% de los pacientes pediátricos, sin diferencias con respecto a los adultos. Únicamente el 16% de los pacientes mostraron efectos adversos, en su mayoría en forma de eritema leve. Encontramos mayor adherencia al tratamiento en los pacientes pediátricos que en los adultos (p < 0,05).
Conclusionesla fototerapia con UVB-BE y/o PUVA parece un tratamiento seguro y eficaz en niños, sin ser necesarios protocolos de tratamiento diferentes a los empleados en adultos. La adherencia al tratamiento es mayor que en los pacientes adultos.
Phototherapy is a technique based on the use of ultraviolet (UV) radiation to treat different skin diseases. Its therapeutic efficacy is due to the following: 1) its anti-inflammatory and immunomodulatory action on different elements of the immune system; 2) inhibition of DNA synthesis and inhibition of keratinocyte proliferation1; and 3) reduction of colonization by Staphylococcus aureus.2 Narrow-band UVB phototherapy (NB-UVB) or UVA phototherapy and psoralen (PUVA) may be used as second-line treatment in a wide variety of skin diseases when topical treatment is insufficient, such as in atopic dermatitis and psoriasis.
The efficacy and safety of phototherapy have been thoroughly established in adults and some publications indicate that it is also an effective and safe treatment in pediatric patients with refractory skin diseases. The principal objective of this study is to review the use of this technique in pediatric patients treated in a tertiary hospital in recent years and to describe the most frequently treated dermatologic diseases and the mode of phototherapy used, together with the number of cycles and the administered dosage. The secondary objectives were to determine whether differences existed in terms of efficacy, safety and methodology in the use of phototherapy compared with adult patients.
Materials and MethodsAll patients under the age of 17 years who were treated with phototherapy at the Department of Pediatric Dermatology of Hospital General Universitario de Valencia, Spain were included in the study. All pediatric patients who received phototherapy between 2002 and December 2017 were included. The phototherapy protocol we used in our patients is that recommended in the consensus statement of the Spanish Photobiology Group, depending on the phototype. The data for these patients was collected retrospectively from their clinical records. The variables of interest were sex, age, skin disease, mode of phototherapy received, number of cycles, number of sessions per cycle, mean cumulative dose (in J/cm2), response to treatment, adverse effects, and whether and why treatment was abandoned.
To evaluate treatment response, complete response was defined as total improvement or complete bleaching of the dermatosis, partial response as improvement of symptoms without achieving complete response, and null response as a complete absence of improvement. Adverse effects were defined as mild if they did not require treatment or suspension of the phototherapy cycle, moderate if topical treatment or reduction of the following dose in the phototherapy cycle was required, or severe if topical or systemic treatment was required and suspension of the phototherapy cycle was necessary.
Furthermore, a cohort of adult patients (over 18 years of age) who underwent phototherapy during the same period of time was selected. The same variables as for the pediatric patients were recorded retrospectively. The t test for independent samples was used to determine the existence of differences between the mean accumulated dose used in children and in adults. The χ2 test was used to determine the existence of differences between children and adults who received NB-UVB and PUVA, those who responded or did not, the presence of adverse effects, and abandonment of treatment. Statistical analysis was performed using version 21.0 of the Statistical Package for Social Sciences.
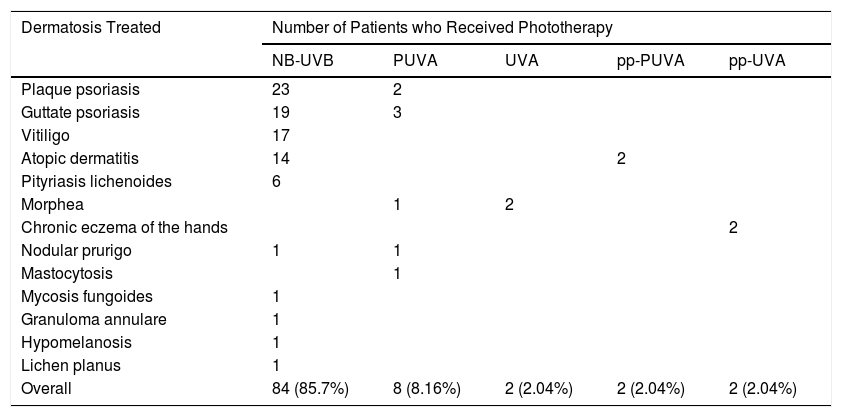
ResultsA total of 95 children (58 [61.1%] girls and 37 [38.9%] boys) were included in the study. The mean age was 10.86 years, with no differences regarding age (P>.05). Seventy-five percent of patients were classified as phototypes II or III on the Fitzpatrick scale. The dermatologic diseases presented by these patients were plaque psoriasis (25%), guttate psoriasis (23%), vitiligo (17%), atopic dermatitis (16%), pityriasis lichenoides (6%), morphea (3%), nodular prurigo (2%), palmoplantar eczema (2%), linear psoriasis (1%), cutaneous mastocytosis (1%), mycosis fungoides (1%), lichen planus (1%), granuloma annulare (1%), and hypomelanosis (1%). A total of 98 different treatment cycles were performed during the follow-up of these patients, of which 86% were NB-UVB, 8% PUVA, 2% UVA, 2% palmoplantar PUVA, and 2% palmoplantar UVA. The modality of phototherapy used according to the pediatric skin disease is shown in Table 1.
Modality of Phototherapy Used by Pediatric Skin Disease Treated.
| Dermatosis Treated | Number of Patients who Received Phototherapy | ||||
|---|---|---|---|---|---|
| NB-UVB | PUVA | UVA | pp-PUVA | pp-UVA | |
| Plaque psoriasis | 23 | 2 | |||
| Guttate psoriasis | 19 | 3 | |||
| Vitiligo | 17 | ||||
| Atopic dermatitis | 14 | 2 | |||
| Pityriasis lichenoides | 6 | ||||
| Morphea | 1 | 2 | |||
| Chronic eczema of the hands | 2 | ||||
| Nodular prurigo | 1 | 1 | |||
| Mastocytosis | 1 | ||||
| Mycosis fungoides | 1 | ||||
| Granuloma annulare | 1 | ||||
| Hypomelanosis | 1 | ||||
| Lichen planus | 1 | ||||
| Overall | 84 (85.7%) | 8 (8.16%) | 2 (2.04%) | 2 (2.04%) | 2 (2.04%) |
Abbreviations: pp indicates palmoplantar; PUVA, psoralen-associated ultraviolet A; NB-UVB, narrow-band ultraviolet B.
A total of 122 randomly selected adult patients (over 18 years of age) were also included: 79 (64.7%) women and 43 (35.3%) men, with a mean age of 51.51 years. These patients underwent a total of 126 different treatments. Of these adult patients, 78.6% were classified as phototypes II or III on the Fitzpatrick scale. The dermatoses presented by these patients were plaque psoriasis (41%), palmoplantar psoriasis (11%), vitiligo (11%), atopic dermatitis (6%), guttate psoriasis (6%), granuloma annulare (6%), nodular prurigo (6%), mycosis fungoides (4%), solar urticaria (2%), palmoplantar eczema (2%), pityriasis lichenoides (2%), lichen planus (2%), and erythema annulare centrifugum (1%). Seventy-five percent of these patients received NB-UVB, 11% received PUVA, and 14% received palmoplantar PUVA. No differences were found between the number of children and adults who received the NB-UVB modality and the PUVA modality of phototherapy (P>.05).
Sixty percent of the pediatric patients received a single cycle of NB-UVB, with a mean of 48.25 sessions per cycle. The mean cumulative dose was 34.92J/cm2, and no significant differences were found with regard to the mean cumulative dose in adults (29.20J/cm2, P>.05). Five of the 7 pediatric patients who received PUVA underwent a single cycle, with a mean of 44.7 sessions per cycle. The mean cumulative dose was 183.71J/cm2, and no significant differences were found with regard to the mean cumulative dose in adults (160.80J/cm2, P>.05).
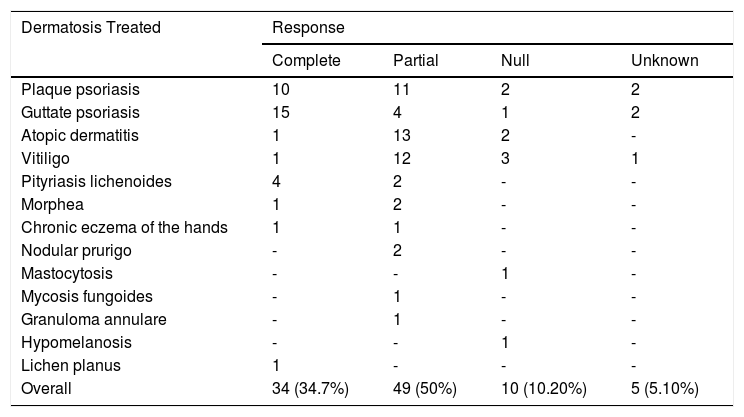
Thirty-five percent of pediatric patients achieved a complete response compared to 36.88% of adult patients; these differences were not statistically significant (P>.05). A partial response was achieved by 50% of the pediatric patients and 10% of them achieved no response (the response was unknown in 5% of patients). The type of response by disease treated is shown in Table 2. The dermatologic diseases that responded best to phototherapy were guttate psoriasis (75% complete response) and pityriasis lichenoides (66% complete response). Of the patients with vitiligo and atopic dermatitis, 81.25% and 87.5%, respectively, showed clinical improvement but not complete clearance.
Type of Response Achieved Depending on the Dermatosis Treated in the Pediatric Population.
| Dermatosis Treated | Response | |||
|---|---|---|---|---|
| Complete | Partial | Null | Unknown | |
| Plaque psoriasis | 10 | 11 | 2 | 2 |
| Guttate psoriasis | 15 | 4 | 1 | 2 |
| Atopic dermatitis | 1 | 13 | 2 | - |
| Vitiligo | 1 | 12 | 3 | 1 |
| Pityriasis lichenoides | 4 | 2 | - | - |
| Morphea | 1 | 2 | - | - |
| Chronic eczema of the hands | 1 | 1 | - | - |
| Nodular prurigo | - | 2 | - | - |
| Mastocytosis | - | - | 1 | - |
| Mycosis fungoides | - | 1 | - | - |
| Granuloma annulare | - | 1 | - | - |
| Hypomelanosis | - | - | 1 | - |
| Lichen planus | 1 | - | - | - |
| Overall | 34 (34.7%) | 49 (50%) | 10 (10.20%) | 5 (5.10%) |
Sixteen percent of pediatric patients showed adverse effects, compared to 22% of adult patients, although these differences were not statistically significant (P>.05). Twelve percent of them showed only mild adverse effects in the form of mild erythema, whereas only one patient showed moderate erythema, which required a reduction of the dosage in the following phototherapy session. Three patients presented vasovagal dizziness during the phototherapy session, which required the session to be suspended.
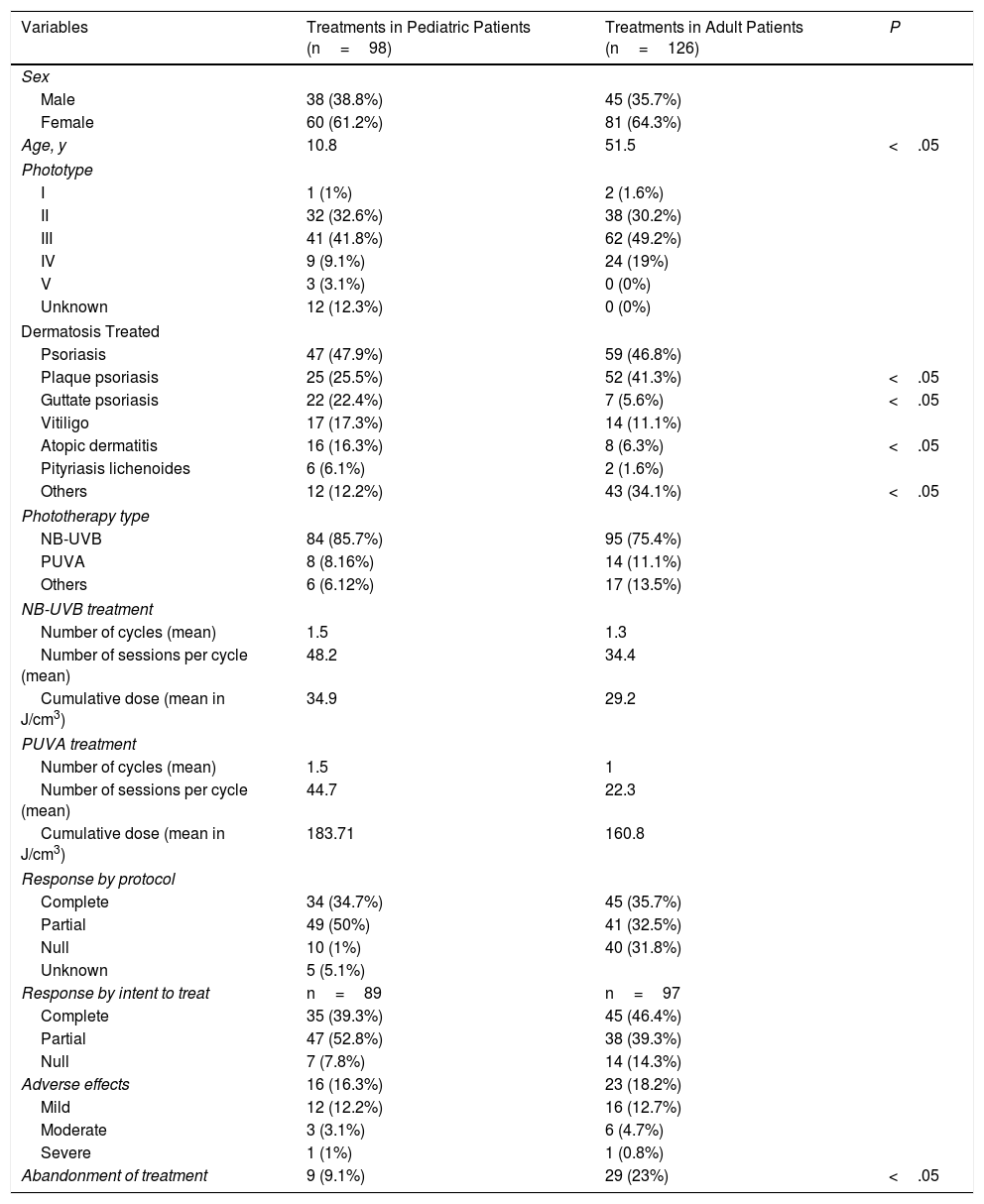
Ninety-three percent of pediatric patients completed the treatment and the most frequent cause of abandonment was incompatibility with school. Two patients stopped attending the sessions and follow-up was lost, and the phototherapy cycle was suspended in one of them due to pregnancy (a 16-year-old patient). Abandonment of treatment was statistically more frequent in adults compared to pediatric patients (P=.006). Table 3 shows the patient characteristics analyzed in the study.
Epidemiological, Clinical, and Methodological Characteristics of the Pediatric and Adult Patients Included in the Study who Received Phototherapy.
| Variables | Treatments in Pediatric Patients (n=98) | Treatments in Adult Patients (n=126) | P |
|---|---|---|---|
| Sex | |||
| Male | 38 (38.8%) | 45 (35.7%) | |
| Female | 60 (61.2%) | 81 (64.3%) | |
| Age, y | 10.8 | 51.5 | <.05 |
| Phototype | |||
| I | 1 (1%) | 2 (1.6%) | |
| II | 32 (32.6%) | 38 (30.2%) | |
| III | 41 (41.8%) | 62 (49.2%) | |
| IV | 9 (9.1%) | 24 (19%) | |
| V | 3 (3.1%) | 0 (0%) | |
| Unknown | 12 (12.3%) | 0 (0%) | |
| Dermatosis Treated | |||
| Psoriasis | 47 (47.9%) | 59 (46.8%) | |
| Plaque psoriasis | 25 (25.5%) | 52 (41.3%) | <.05 |
| Guttate psoriasis | 22 (22.4%) | 7 (5.6%) | <.05 |
| Vitiligo | 17 (17.3%) | 14 (11.1%) | |
| Atopic dermatitis | 16 (16.3%) | 8 (6.3%) | <.05 |
| Pityriasis lichenoides | 6 (6.1%) | 2 (1.6%) | |
| Others | 12 (12.2%) | 43 (34.1%) | <.05 |
| Phototherapy type | |||
| NB-UVB | 84 (85.7%) | 95 (75.4%) | |
| PUVA | 8 (8.16%) | 14 (11.1%) | |
| Others | 6 (6.12%) | 17 (13.5%) | |
| NB-UVB treatment | |||
| Number of cycles (mean) | 1.5 | 1.3 | |
| Number of sessions per cycle (mean) | 48.2 | 34.4 | |
| Cumulative dose (mean in J/cm3) | 34.9 | 29.2 | |
| PUVA treatment | |||
| Number of cycles (mean) | 1.5 | 1 | |
| Number of sessions per cycle (mean) | 44.7 | 22.3 | |
| Cumulative dose (mean in J/cm3) | 183.71 | 160.8 | |
| Response by protocol | |||
| Complete | 34 (34.7%) | 45 (35.7%) | |
| Partial | 49 (50%) | 41 (32.5%) | |
| Null | 10 (1%) | 40 (31.8%) | |
| Unknown | 5 (5.1%) | ||
| Response by intent to treat | n=89 | n=97 | |
| Complete | 35 (39.3%) | 45 (46.4%) | |
| Partial | 47 (52.8%) | 38 (39.3%) | |
| Null | 7 (7.8%) | 14 (14.3%) | |
| Adverse effects | 16 (16.3%) | 23 (18.2%) | |
| Mild | 12 (12.2%) | 16 (12.7%) | |
| Moderate | 3 (3.1%) | 6 (4.7%) | |
| Severe | 1 (1%) | 1 (0.8%) | |
| Abandonment of treatment | 9 (9.1%) | 29 (23%) | <.05 |
In this study, we have observed that phototherapy is an effective and safe treatment in pediatric patients, and shows good adherence to treatment. It may be indicated as a second line treatment when topical treatment fails. Table 3 shows how the skin diseases treated in the adult population are more varied than in the pediatric population, which entails other treatments (for example, palmoplantar PUVA for palmoplantar psoriasis).
In our study, the most frequently treated diseases were psoriasis, vitiligo, and atopic dermatitis. We also considered plaque psoriasis and guttate psoriasis as separate entities, as the literature contains evidence regarding clinical and prognostic differences between these entities.3 The skin diseases most frequently treated with phototherapy in our study differ partly from those published in the literature, where atopic dermatitis tends to be the most commonly treated disease.4 This is probably because atopic dermatitis courses with outbreaks, which can be controlled with emollients and topical treatments, or even with a short course of systemic corticosteroids, with phototherapy reserved for patients with recalcitrant diseases that are prolonged over time.5 Furthermore, atopic dermatitis improves with the age of the patient and many patients who receive phototherapy for this condition are therefore adults.6 Moreover, because psoriasis is a more stable disease over time, we tend to use a scaled treatment and, when topical treatments fail, we consider starting children on phototherapy before classical systemic therapy.
We observed a complete clearance rate of 35% and a general improvement rate of 85% in our pediatric patients. The response depends largely on the disease treated. Of the children with plaque psoriasis and guttate psoriasis, 43% and 75%, respectively, showed a complete response to phototherapy (not counting those for whom the information on treatment response is not known). No significant differences were found in terms of number of sessions (35 vs 36; P=.8) and mean cumulative dose (47 vs 59.3; P=.5) used in patients with plaque psoriasis and guttate psoriasis, respectively. We have found no studies in the literature that separate these two entities, as psoriasis is considered as a single entity. The response rate is similar to that published in other studies. Tan et al7 report a response rate (considered as an improvement of≥75% in their dermatosis) of 90%, somewhat higher than in our study. Eustace et al4 treated 21 patients with psoriasis with NB-UVB, of which 15 completed treatment. Those authors reported a clearance rate of 86%. Pavlosky et al8 reported a 51% rate of complete response and a 41% rate of good response.
Of our pediatric patients with atopic dermatitis, 87.5% responded to treatment but without achieving a complete response. This efficacy is somewhat greater than that published in other studies of pediatric patients. Tan et al reported an improvement of 75% or more in 71% of their patients with atopic dermatitis treated with phototherapy,7 similar to the rates found by Eustace et al,4 who reported that 76% of their 33 patients with atopic dermatitis achieved a complete or almost complete response.
The response of patients with vitiligo treated with phototherapy is perhaps more difficult to evaluate. While this is a disease that responds poorly to different treatments, we found a clinical improvement rate of 81.25% (in 13 of 16 children who completed treatment). The literature shows highly variable results, with improvement rates of 75% or greater in 45.4% of patients treated,9 or even patients who achieve spectacular improvement with almost complete repigmentation.4 Other subtypes of phototherapy, such as high-intensity targeted ultraviolet B light (304-312nm), have shown good therapeutic efficacy and good tolerance.10
Also of note are the mean accumulated doses used in our pediatric patients treated with NB-UVB and PUVA, which were 34.92J/cm2 and 183.71J/cm2, respectively. These doses are similar to those reported in other studies.11 We also found no significant differences with respect to the mean accumulated doses reported in adult patients. This suggests that it is not necessary to modify the protocols or that it is not necessary to use different protocols when using this technique in pediatric patients.
Phototherapy is one of the safest treatments we can use in pediatric patients. We found that only 16% of the children showed adverse effects, mostly in the form of mild erythema. The degree of secondary erythema depends on the phototype of the patients, the dose used, and dose increments. Eustace et al4 report rates of mild erythema of 37.5% and 23.8% in children with atopic dermatitis and psoriasis, respectively. This is higher than the rate found in our study, owing to the fact that 69% of their patients were phototype I and II compared to 75% of our patients, who were classified as phototypes II and III. The rate of adverse effects in other studies is similar to that found in our study.12
Also of note is the high rate of adherence to this treatment in our study, which is higher than that for adult patients. This is because our nursing service organized patients receiving phototherapy by reserving sessions for the first appointments in the morning or at mid-morning for pediatric patients, so that they could attend before going to school or during their morning break.
We are aware of the limitations of our study. First, the loss of data typical of a retrospective study means that we cannot exactly determine the response of some patients to the phototherapy. While scales exist that assess the degree of involvement and improvement in different diseases, they are not widely used in daily clinical practice. Finally, we do not have medium-term or long-term follow-up of these patients and therefore do not know the relapse rates or long-term effects due to the potential risk of malignancy from phototherapy.13
In conclusion, phototherapy is an effective and safe treatment in pediatric patients with different diseases. The response depends essentially on the disease treated. The accumulated dose is no different from that used in adult patients. The treatment has a low rate of adverse effects, which are mostly mild, and has a high rate of treatment adherence—greater than that found in adult patients.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
Please cite this article as: Jorge M-T, Valenzuela-Oñate MaríaO-SJ, , Cristian, Pedro M-C, Altea E-M, et al. Experiencia en el uso de fototerapia en pacientes pediátricos y comparación de esta técnica frente a pacientes adultos. Actas Dermosifiliogr. 2020;111:41–46.



